

Tuberculosis attributed to transmission within healthcare facilities, Botswana-The Kopanyo Study
- PMID: 35382909
- PMCID: PMC9535034
- DOI: 10.1017/ice.2021.517
Tuberculosis attributed to transmission within healthcare facilities, Botswana-The Kopanyo Study
Abstract
Objective: Healthcare facilities are a well-known high-risk environment for transmission of M. tuberculosis, the etiologic agent of tuberculosis (TB) disease. However, the link between M. tuberculosis transmission in healthcare facilities and its role in the general TB epidemic is unknown. We estimated the proportion of overall TB transmission in the general population attributable to healthcare facilities.
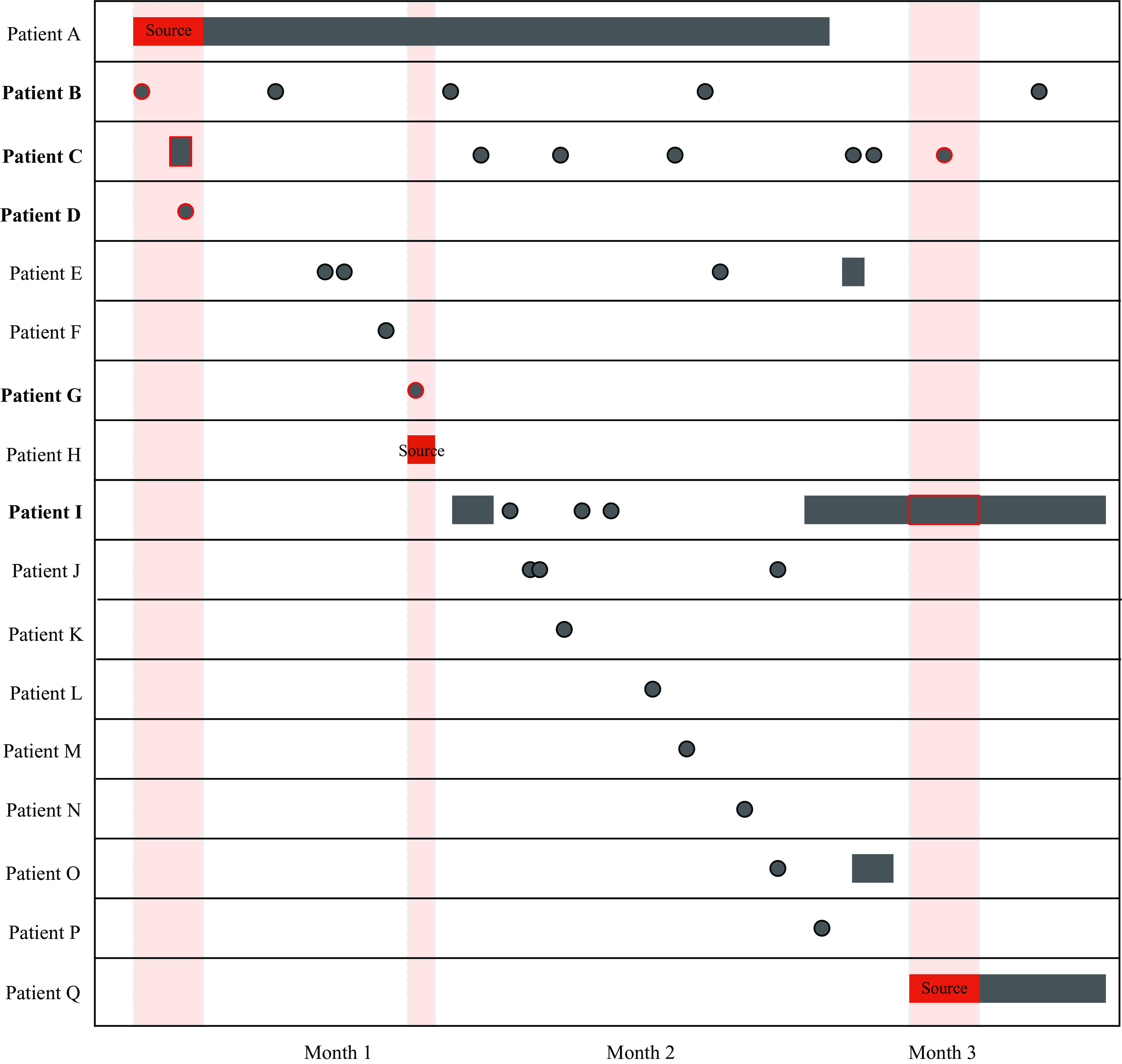
Methods: We combined data from a prospective, population-based molecular epidemiologic study with a universal electronic medical record (EMR) covering all healthcare facilities in Botswana to identify biologically plausible transmission events occurring at the healthcare facility. Patients with M. tuberculosis isolates of the same genotype visiting the same facility concurrently were considered an overlapping event. We then used TB diagnosis and treatment data to categorize overlapping events into biologically plausible definitions. We calculated the proportion of overall TB cases in the cohort that could be attributable to healthcare facilities.
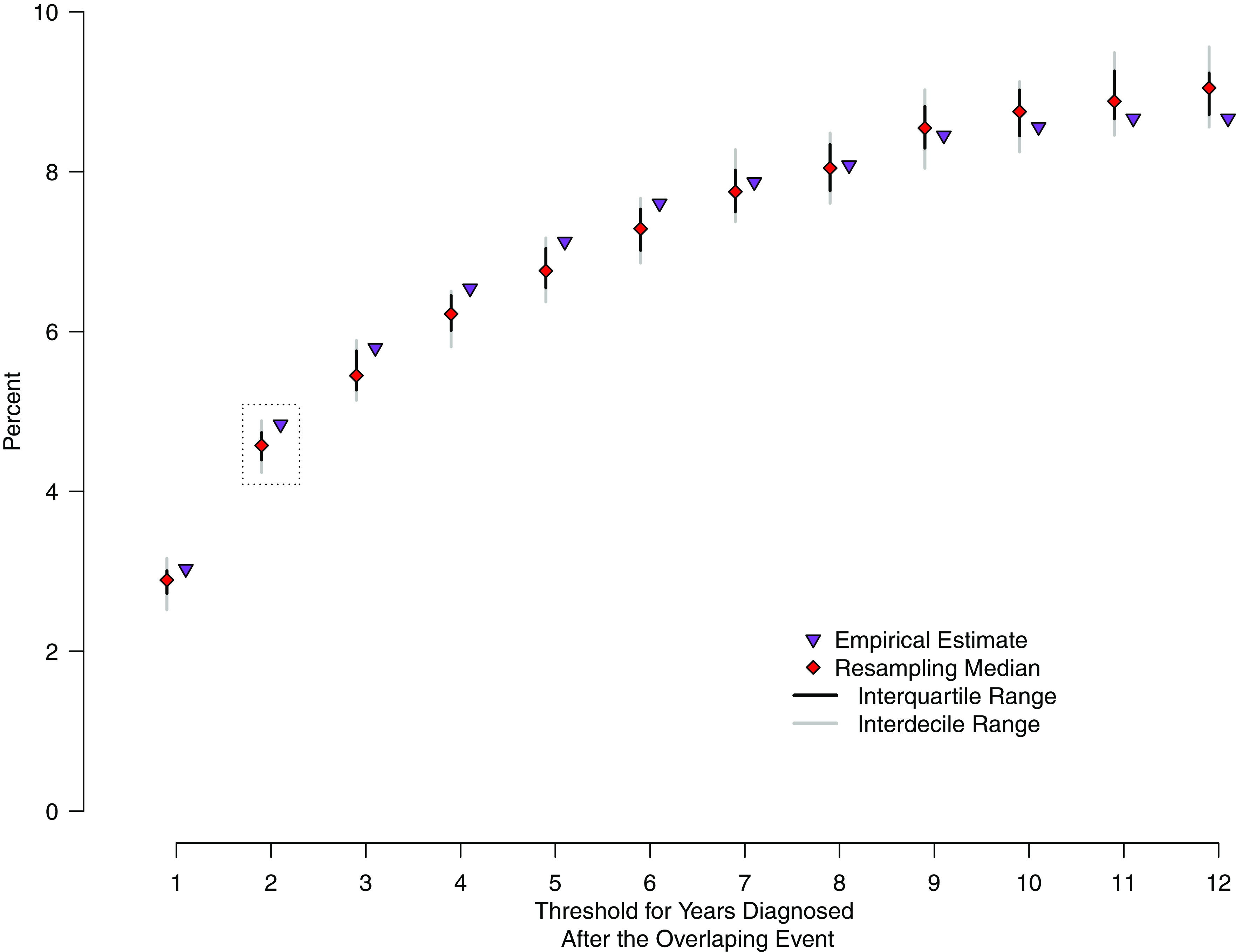
Results: In total, 1,881 participants had TB genotypic and EMR data suitable for analysis, resulting in 46,853 clinical encounters at 338 healthcare facilities. We identified 326 unique overlapping events involving 370 individual patients; 91 (5%) had biologic plausibility for transmission occurring at a healthcare facility. A sensitivity analysis estimated that 3%-8% of transmission may be attributable to healthcare facilities.
Conclusions: Although effective interventions are critical in reducing individual risk for healthcare workers and patients at healthcare facilities, our findings suggest that development of targeted interventions aimed at community transmission may have a larger impact in reducing TB.
Keywords: Tuberculosis; healthcare facilities; nosocomial transmission; transmission.
Figures
References
-
- Global Tuberculosis Report. Geneva: World Health Organization; 2021.
-
- Apriani L, McAllister S, Sharples K, et al. Latent tuberculosis infection in healthcare workers in low- and middle-income countries: an updated systematic review. Eur Respir J 2019;53:1801789. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
