

Gain-of-function and loss-of-function GABRB3 variants lead to distinct clinical phenotypes in patients with developmental and epileptic encephalopathies
- PMID: 35383156
- PMCID: PMC8983652
- DOI: 10.1038/s41467-022-29280-x
Gain-of-function and loss-of-function GABRB3 variants lead to distinct clinical phenotypes in patients with developmental and epileptic encephalopathies
Abstract
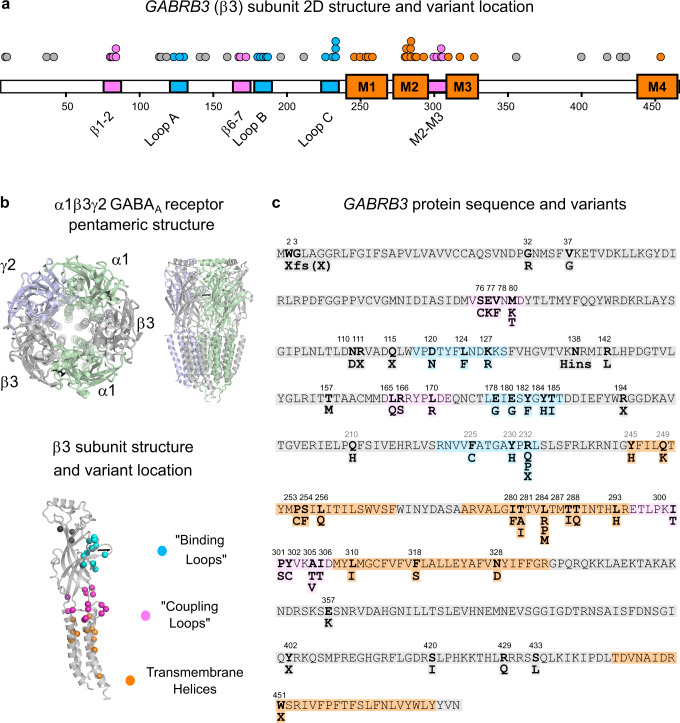
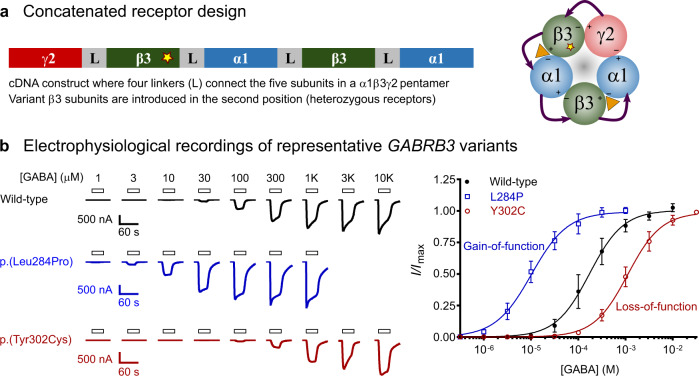
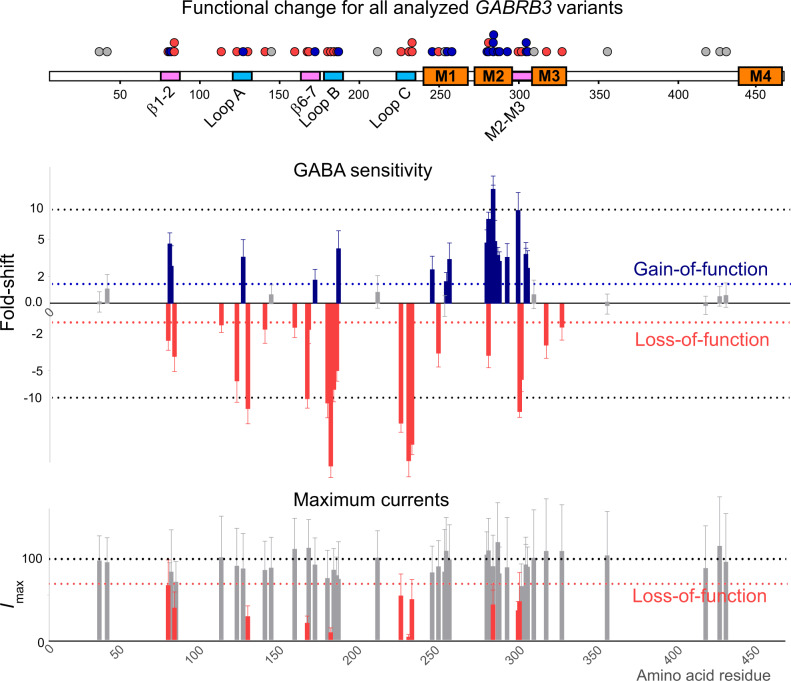
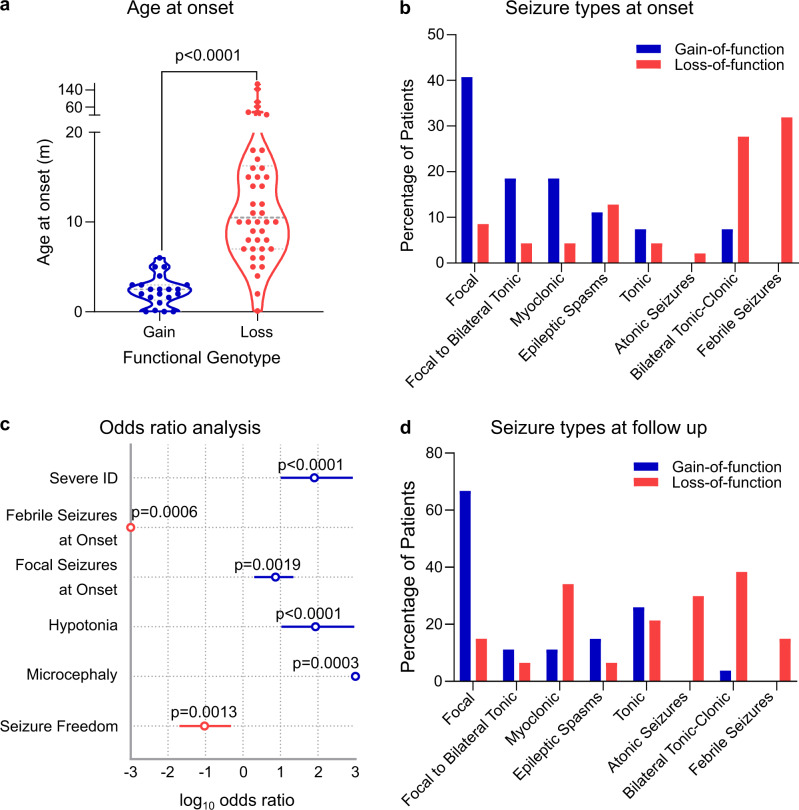
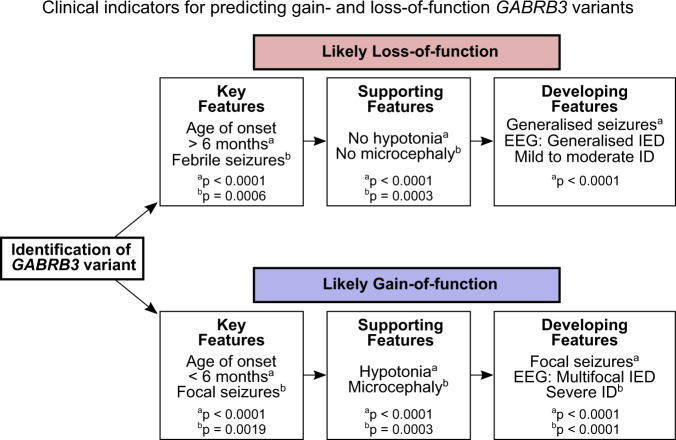
Many patients with developmental and epileptic encephalopathies present with variants in genes coding for GABAA receptors. These variants are presumed to cause loss-of-function receptors leading to reduced neuronal GABAergic activity. Yet, patients with GABAA receptor variants have diverse clinical phenotypes and many are refractory to treatment despite the availability of drugs that enhance GABAergic activity. Here we show that 44 pathogenic GABRB3 missense variants segregate into gain-of-function and loss-of-function groups and respective patients display distinct clinical phenotypes. The gain-of-function cohort (n = 27 patients) presented with a younger age of seizure onset, higher risk of severe intellectual disability, focal seizures at onset, hypotonia, and lower likelihood of seizure freedom in response to treatment. Febrile seizures at onset are exclusive to the loss-of-function cohort (n = 47 patients). Overall, patients with GABRB3 variants that increase GABAergic activity have more severe developmental and epileptic encephalopathies. This paradoxical finding challenges our current understanding of the GABAergic system in epilepsy and how patients should be treated.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Comment in
-
No Gain, Less Pain: GABRB3 Mutations in Epileptic Encephalopathy.Epilepsy Curr. 2022 Nov 1;23(1):44-46. doi: 10.1177/15357597221130199. eCollection 2023 Jan-Feb. Epilepsy Curr. 2022. PMID: 36923344 Free PMC article. No abstract available.
References
-
- Heyne HO, et al. De novo variants in neurodevelopmental disorders with epilepsy. Nat. Genet. 2018;50:1048–1053. - PubMed
-
- Hernandez CC, Macdonald RL. A structural look at GABAA receptor mutations linked to epilepsy syndromes. Brain Res. 2019;1714:234–247. - PubMed
-
- Maljevic S, et al. Spectrum of GABAA receptor variants in epilepsy. Curr. Opin. Neurol. 2019;32:183–190. - PubMed
-
- Myers KA, et al. Contribution of rare genetic variants to drug response in absence epilepsy. Epilepsy Res. 2021;170:106537. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
