

An Update on Refractory Hypertension
- PMID: 35384577
- PMCID: PMC9300497
- DOI: 10.1007/s11906-022-01185-6
An Update on Refractory Hypertension
Abstract
Purpose of review: To update on definition, diagnosis, prevalence, patient characteristics, pathophysiology, and treatment of refractory hypertension (RfHTN).
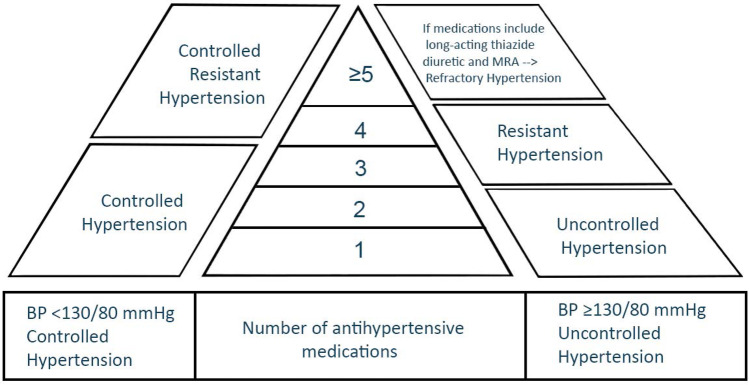
Recent findings: Refractory hypertension (RfHTN) is defined as blood pressure (BP) that is uncontrolled despite using ≥ 5 antihypertensive medications of different classes, including a long-acting thiazide diuretic and a mineralocorticoid receptor antagonist (MRA) at maximal or maximally tolerated doses. This new phenotype is different from resistant hypertension (RHTN), defined as BP that is uncontrolled despite using ≥ 3 medications, commonly a long-acting calcium channel blocker (CCB), a blocker of the renin-angiotensin system (angiotensin-converting enzyme [ACE] inhibitor or angiotensin receptor blocker [ARB]), and a diuretic. The RHTN phenotype includes controlled RHTN, BP that is controlled on 4 or more medications. RfHTN is largely attributable to increased sympathetic activity, unlike RHTN, which is mainly due to increased intravascular fluid volume frequently caused by hyperaldosteronism and chronic excessive sodium ingestion. Compared to those with controlled RHTN, patients with RfHTN have a higher prevalence of target organ damage and do not have elevated aldosterone levels. Ongoing clinical trials are assessing the safety and efficacy of using devices to aid with BP control in patients with RfHTN. RfHTN is a separate entity from RHTN and is generally attributable to increased sympathetic activity.
Keywords: Primary aldosteronism; Renal denervation; Sleep apnea; Spironolactone; Sympathetic activation.
© 2022. The Author(s).
Conflict of interest statement
Faris Matanes reports grants from NIH during the conduct of the study. Suzanne Oparil declares the following Editor-in-Chief, Current Hypertension Reports (Journal; Publisher – Springer Science Business Media LLC); annual stipend of $5,000 (Springer); Editor-in-Chief Term until 12/2022. M. Bilal Khan, Mohammed Siddiqui, Tanja Dudenbostel, and David Calhoun declare that they have no conflict of interest.
Figures
References
-
- •• Carey RM, Calhoun DA, Bakris GL, Brook RD, Daugherty SL, Dennison-Himmelfarb CR, et al. Resistant hypertension: detection, evaluation, and management: a scientific statement from the American Heart Association. Hypertension. 2018;72(5):e53-e90. 10.1161/hyp.0000000000000084. This scientific statement provides a comprehensive approach to properly define RHTN, identify secondary causes of HTN, and describe the appropriate treatment of RHTN. - PMC - PubMed
-
- Gaddam KK, Nishizaka MK, Pratt-Ubunama MN, Pimenta E, Aban I, Oparil S, et al. Characterization of resistant hypertension: association between resistant hypertension, aldosterone, and persistent intravascular volume expansion. Arch Intern Med. 2008 doi: 10.1001/archinte.168.11.1159. - DOI - PMC - PubMed
-
- • Williams B, MacDonald TM, Morant S, Webb DJ, Sever P, McInnes G, et al. Spironolactone versus placebo, bisoprolol, and doxazosin to determine the optimal treatment for drug-resistant hypertension (PATHWAY-2): a randomised, double-blind, crossover trial. Lancet. 2015;386(10008):2059–68. 10.1016/S0140-6736(15)00257-3. This trial illustrates the superiority of spironolactone for treatment of RHTN and the degree of BP reduction based on renin levels. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
