

Iron Deficiency in Patients with Inflammatory Bowel Diseases: A Prospective Multicenter Cross-Sectional Study
- PMID: 35384624
- PMCID: PMC9652270
- DOI: 10.1007/s10620-022-07474-z
Iron Deficiency in Patients with Inflammatory Bowel Diseases: A Prospective Multicenter Cross-Sectional Study
Abstract
Background: Iron deficiency (ID) is a frequent condition in patients with inflammatory bowel disease (IBD).
Aim: Our aim was to investigate the prevalence of ID in patients with IBD.
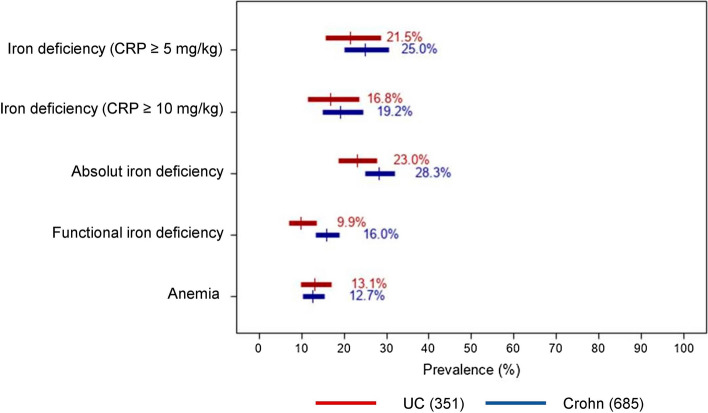
Methods: This was a prospective multicenter cross-sectional study conducted in 21 gastroenterology departments in France between January and March 2020. All adult patients with confirmed IBD who were admitted to the hospital were eligible for inclusion. ID was defined as ferritinemia ≤ 100 μg/L in patients with signs of inflammation (C-reactive protein (CRP) ≥ 5 mg/L) or ferritinemia < 30 μg/L in the absence of inflammation.
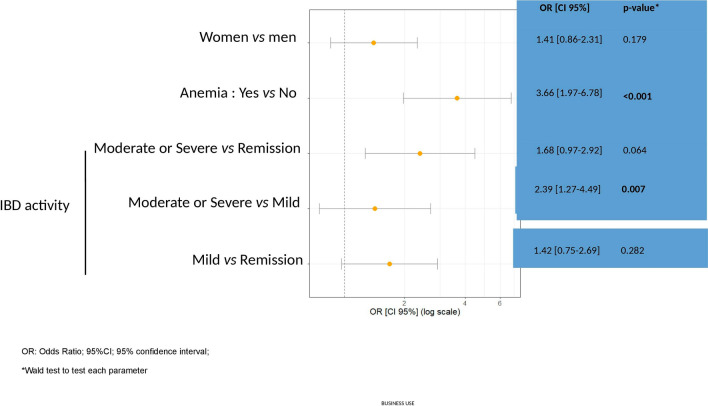
Results: In total, 1036 IBD (685 Crohn's disease and 351 ulcerative colitis) patients (52.1% women) with a mean age of 41.8 ± 15.5 years were recruited. Approximately half of the patients (504, 51.1%) were in disease remission at the time of enrollment. Systematic monitoring of iron status was performed in 12/21 (57%) participating centers, including measurements of ferritin (12/12, 100%), hemoglobin (11/12, 92%), transferrin saturation (TSAT) (6/12, 50.0%), and serum iron (5/12, 42%). About one-fifth of the patients had been treated with intravenous iron (218, 21.0%), whereas only a small percentage received oral iron (36, 3.5%). ID occurred in 97 patients (23.7% CI 95% 19.8-28.1). Patients with moderate/severe IBD activity (OR: 3.66; CI 95% 24.4-61.2; p = 0.007) or concomitant anemia (OR: 3.66; CI 95% 1.97-6.78; p < 0.001) had an increased likelihood of having ID.
Conclusion: Patients with moderate/severe IBD activity or concomitant anemia are at increased risk of ID. Early detection and management of ID in patients with IBD is recommended.
Keywords: Crohn’s disease; Inflammatory bowel disease; Iron deficiency; Prevalence; Ulcerative colitis.
© 2022. The Author(s).
Conflict of interest statement
L Peyrin-Biroulet reports personal fees from Galapagos, AbbVie, Janssen, Genentech, Ferring, Tillots, Celltrion, Takeda, Pfizer, Index Pharmaceuticals, Sandoz, Celgene, Biogen, Samsung Bioepis, Inotrem, Allergan, MSD, Roche, Arena, Gilead, Amgen, BMS, Vifor, Norgine, Mylan, Lilly, Fresenius Kabi, OSE Immunotherapeutics, Enthera, Theravance, Pandion Therapeutics, Gossamer Bio, Viatris, and Thermo Fisher; -Grants from Abbvie, MSD, Takeda, and Fresenius Kabi; and stock options from CTMA. G Bouguen received lecture fees from Abbvie, Ferring, MSD, Takeda, and Pfizer and consultant fees from Takeda and Janssen. D Laharie declares counseling, boards, transports or fees from Abbvie, Biogaran, Biogen, Ferring, HAC Pharma, Janssen, MSD, Novartis, Pfizer, Prometheus, Roche, Takeda, Theradiag and Tillots. G Savoye has received lecture fees from Vifor Pharma, Takeda, Pfizer, HAC Pharma, Abbvie, MSD, and Ferring France. This author has also received travel accommodations from Ferring, Abbvie, and MSD France as well as a research grant from Ferring. C Giletta has received lecture/consulting fees from Abbvie, Takeda, Pfizer, Celltrion, and Janssen. C Michiels received lecture fees from MSD and Abbvie and invitations to congresses form MSD, Abbvie and Ferring. M Fumery received lecture and consultant fees form Abbvie, MSD, Takeda, Janssen, Celgene, Boehringer, Biogen, Amgen, Celltrion, Pfizer, Galapagos and Lilly. A. Buisson disclosed consulting fees for Abbvie, Amgen, Arena, Biogen, Celltrion, CTMA, Ferring, Janssen, MSD, Nexbiome, Pfizer, Roche, Takeda, and Tillots, as well as lecture fees for Abbvie, Amgen, Biogen, Janssen, Mayoly-Spindler, MSD, Norgine Pfizer, Roche, Takeda, Tillots, and Vifor Pharma. P. Cacoub received consultancies and honoraria from Vifor Pharma.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
