

High Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Household Transmission Rates Detected by Dense Saliva Sampling
- PMID: 35385575
- PMCID: PMC9047155
- DOI: 10.1093/cid/ciac261
High Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Household Transmission Rates Detected by Dense Saliva Sampling
Abstract
Background: Understanding the dynamics of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) household transmission is important for adequate infection control measures in this ongoing pandemic.
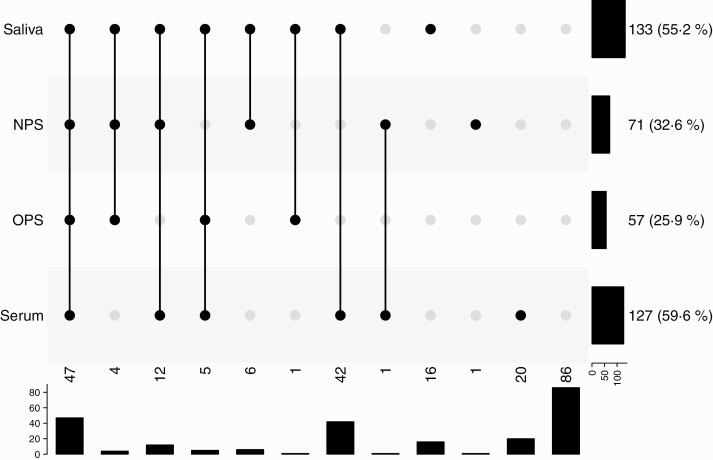
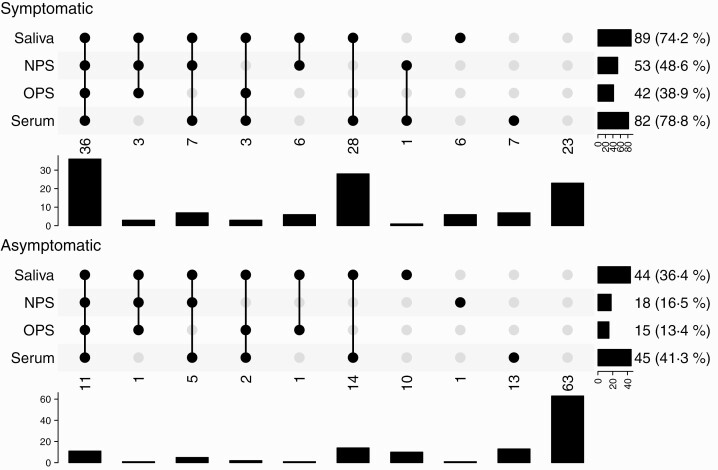
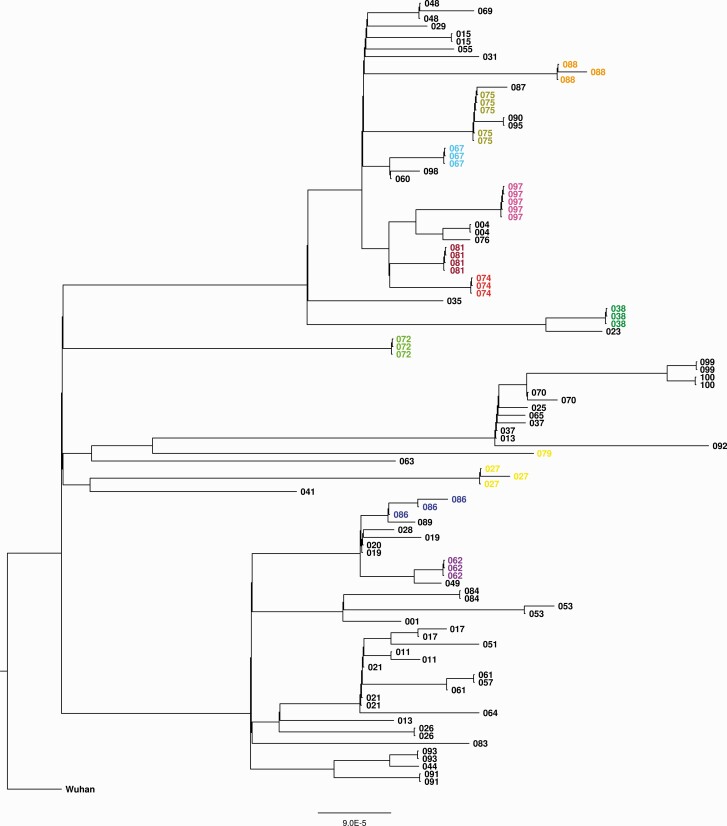
Methods: Households were enrolled upon a polymerase chain reaction-confirmed index case between October and December 2020, prior to the coronavirus disease 2019 vaccination program. Saliva samples were obtained by self-sampling at days 1, 3, 5, 7, 10, 14, 21, 28, 35, and 42 from study inclusion. Nasopharyngeal swabs (NPS) and oropharyngeal swabs (OPS) were collected by the research team at day 7 and capillary blood samples at day 42. Household secondary attack rate (SAR) and per-person SAR were calculated based on at least 1 positive saliva, NPS, OPS, or serum sample. Whole genome sequencing was performed to investigate the possibility of multiple independent SARS-CoV-2 introductions within a household.
Results: Eighty-five households were included consisting of 326 (unvaccinated) individuals. Comparable numbers of secondary cases were identified by saliva (133/241 [55.2%]) and serum (127/213 [59.6%]). The household SAR was 88.2%. The per-person SAR was 64.3%. The majority of the secondary cases tested positive in saliva at day 1 (103/150 [68.7%]). Transmission from index case to household member was not affected by age or the nature of their relationship. Phylogenetic analyses suggested a single introduction for the investigated households.
Conclusions: Households have a pivotal role in SARS-CoV-2 transmission. By repeated saliva self-sampling combined with NPS, OPS, and serology, we found the highest SARS-CoV-2 household transmission rates reported to date. Salivary (self-) sampling of adults and children is suitable and attractive for near real-time monitoring of SARS-CoV-2 transmission in this setting.
Keywords: COVID-19; SARS-CoV-2; household transmission; saliva.
© The Author(s) 2022. Published by Oxford University Press for the Infectious Diseases Society of America.
Figures
References
-
- Center for Systems Science and Engineering, Johns Hopkins University. COVID-19 dashboard. Available at: https://coronavirus.jhu.edu/map.html. Accessed 28 October 2021.
-
- Centers for Disease Control and Prevention. Interim guidelines for collecting and handling of clinical specimens for COVID-19 testing. Available at: https://www.cdc.gov/coronavirus/2019-ncov/lab/guidelines-clinical-specim.... Accessed 1 July 2021.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
