

FcγR-mediated SARS-CoV-2 infection of monocytes activates inflammation
- PMID: 35385861
- PMCID: PMC10071495
- DOI: 10.1038/s41586-022-04702-4
FcγR-mediated SARS-CoV-2 infection of monocytes activates inflammation
Abstract
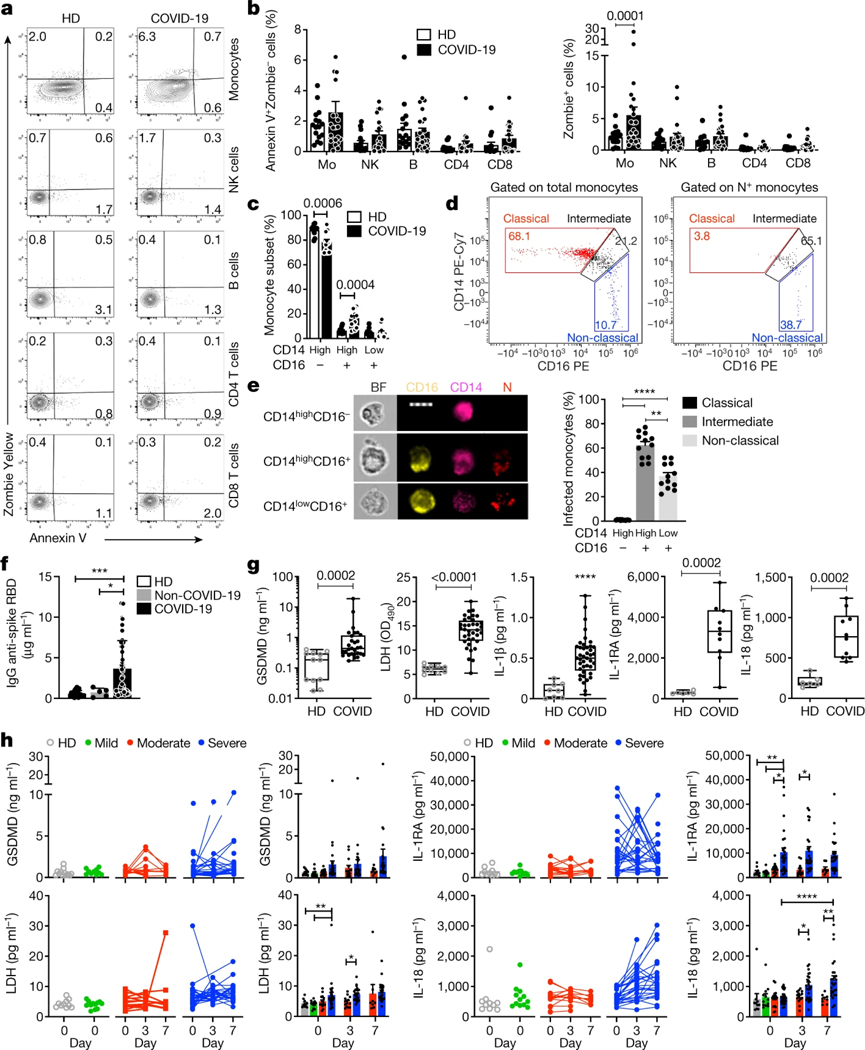
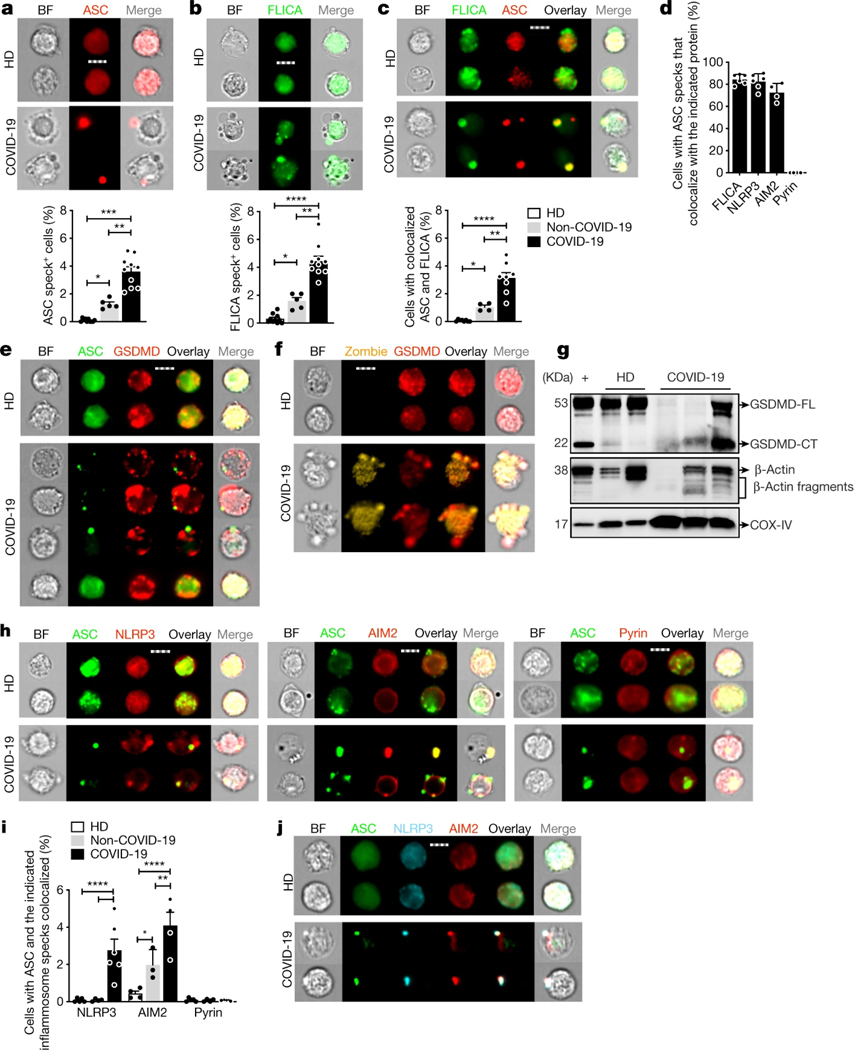
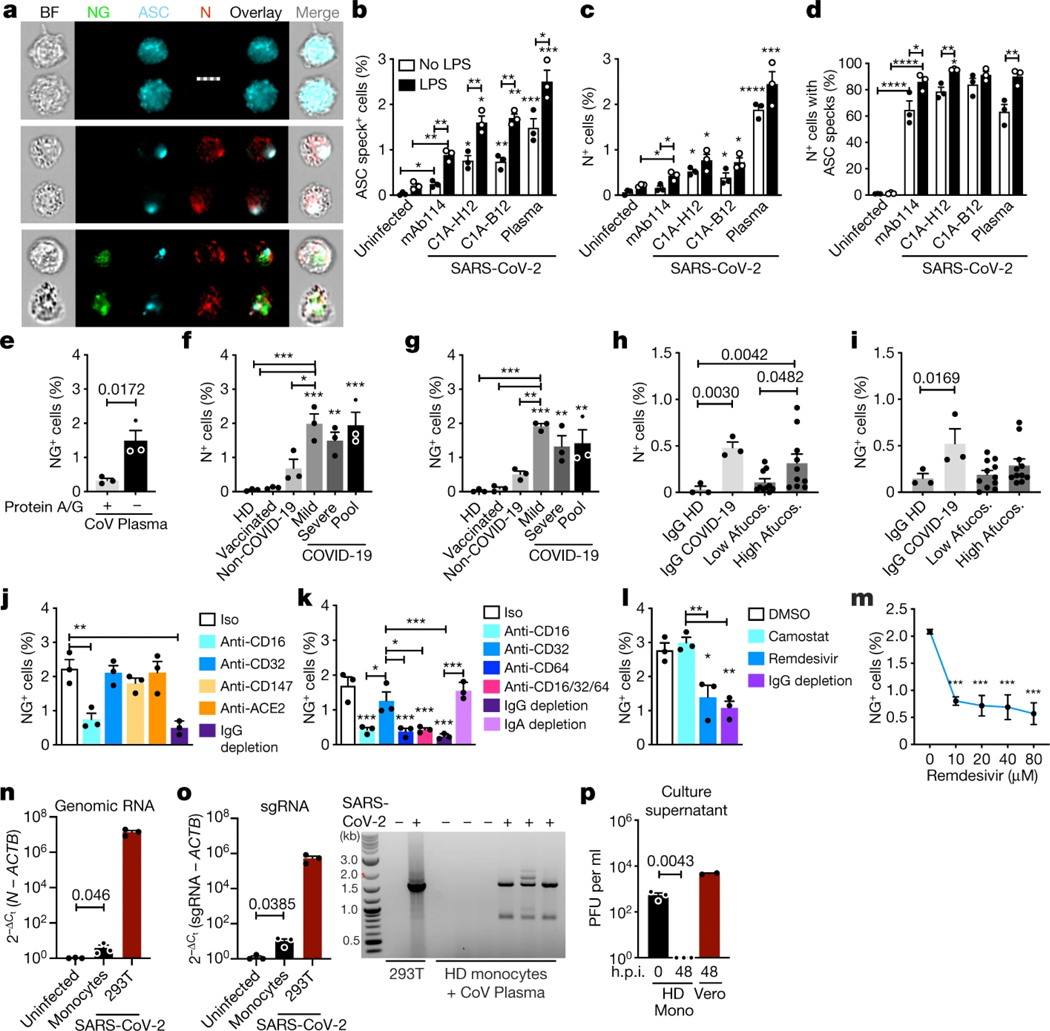
SARS-CoV-2 can cause acute respiratory distress and death in some patients1. Although severe COVID-19 is linked to substantial inflammation, how SARS-CoV-2 triggers inflammation is not clear2. Monocytes and macrophages are sentinel cells that sense invasive infection to form inflammasomes that activate caspase-1 and gasdermin D, leading to inflammatory death (pyroptosis) and the release of potent inflammatory mediators3. Here we show that about 6% of blood monocytes of patients with COVID-19 are infected with SARS-CoV-2. Monocyte infection depends on the uptake of antibody-opsonized virus by Fcγ receptors. The plasma of vaccine recipients does not promote antibody-dependent monocyte infection. SARS-CoV-2 begins to replicate in monocytes, but infection is aborted, and infectious virus is not detected in the supernatants of cultures of infected monocytes. Instead, infected cells undergo pyroptosis mediated by activation of NLRP3 and AIM2 inflammasomes, caspase-1 and gasdermin D. Moreover, tissue-resident macrophages, but not infected epithelial and endothelial cells, from lung autopsies from patients with COVID-19 have activated inflammasomes. Taken together, these findings suggest that antibody-mediated SARS-CoV-2 uptake by monocytes and macrophages triggers inflammatory cell death that aborts the production of infectious virus but causes systemic inflammation that contributes to COVID-19 pathogenesis.
© 2022. The Author(s), under exclusive licence to Springer Nature Limited.
Figures


Update of
-
SARS-CoV-2 infects blood monocytes to activate NLRP3 and AIM2 inflammasomes, pyroptosis and cytokine release.Res Sq [Preprint]. 2021 Aug 11:rs.3.rs-153628. doi: 10.21203/rs.3.rs-153628/v1. Res Sq. 2021. Update in: Nature. 2022 Jun;606(7914):576-584. doi: 10.1038/s41586-022-04702-4. PMID: 34401873 Free PMC article. Updated. Preprint.
Comment in
-
Insights into how SARS-CoV2 infection induces cytokine storms.Trends Immunol. 2022 Jun;43(6):417-419. doi: 10.1016/j.it.2022.04.007. Epub 2022 May 7. Trends Immunol. 2022. PMID: 35537983 Free PMC article.
-
SARS-CoV-2 infection of monocytes: balancing acts of antibodies and inflammasomes.Signal Transduct Target Ther. 2022 Jul 23;7(1):250. doi: 10.1038/s41392-022-01112-w. Signal Transduct Target Ther. 2022. PMID: 35871170 Free PMC article. No abstract available.
References
-
- Akbar AN & Gilroy DW Aging immunity may exacerbate COVID-19. Science 369, 256–257 (2020). - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
