

Management of brain metastasis. Surgical resection versus stereotactic radiotherapy: a meta-analysis
- PMID: 35386568
- PMCID: PMC8982204
- DOI: 10.1093/noajnl/vdac033
Management of brain metastasis. Surgical resection versus stereotactic radiotherapy: a meta-analysis
Abstract
Background: Treatment of metastatic brain tumors often involves radiotherapy with or without surgical resection as the first step. However, the indications for when to use surgery are not clearly defined for certain tumor sizes and multiplicity. This study seeks to determine whether resection of brain metastases versus exclusive radiotherapy provided improved survival and local control in cases where metastases are limited in number and diameter.
Methods: According to PRISMA guidelines, this meta-analysis compares outcomes from treatment of a median number of brain metastases ≤ 4 with a median diameter ≤ 4 cm with exclusive radiotherapy versus surgery followed by radiotherapy. Four randomized control trials and 11 observational studies (1693 patients) met inclusion criteria. For analysis, studies were grouped based on whether radiation involved stereotactic radiosurgery (SRS) or whole-brain radiotherapy (WBRT).
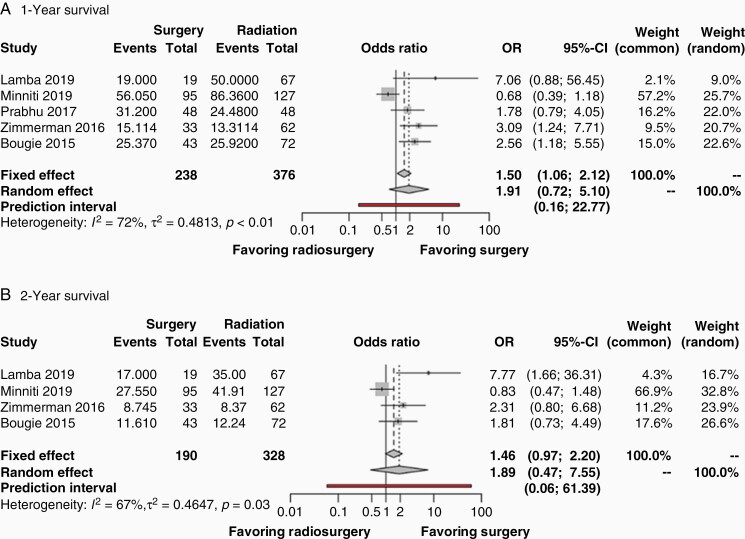
Results: In both analyses, there was no difference in survival between surgery ± SRS versus SRS alone two years after treatment (OR 1.89 (95% CI: 0.47-7.55, P = .23) or surgery + WBRT versus radiotherapy alone (either WBRT and/or SRS) (OR 1.18 (95% CI: 0.76-1.84, P = .46). However, surgical patients demonstrated greater risk for local tumor recurrence compared to SRS alone (OR 2.20 (95% CI: 1.49-3.25, P < .0001)) and compared to WBRT/SRS (OR 2.93; 95% CI: 1.68-5.13, P = .0002).
Conclusion: The higher incidence of local tumor recurrence for surgical patients suggests that more prospective studies are needed to clarify outcomes for treatment of 1-4 metastasis less than 4 cm diameter.
Keywords: brain metastasis; local tumor control; meta-analysis; stereotactic radiotherapy; surgical resection.
© The Author(s) 2022. Published by Oxford University Press, the Society for Neuro-Oncology and the European Association of Neuro-Oncology.
Figures



References
-
- Achrol AS, Rennert RC, Anders C, et al. . Brain metastases. Nat Rev Dis Primers. 2019;5(1):1–26. - PubMed
-
- Suki D, Aziz Hatiboglu M, Sawaya R. Evolution of neurosurgical treatment for brain metastases over a 20-Year period: experience at a large referral cancer center. Neurosurg. 2020;67(Supplement_1):19–28.
-
- Patchell RA, Tibbs PA, Walsh JW, et al. . A randomized trial of surgery in the treatment of single metastases to the brain. N Engl J Med. 1990;322(8):494–500. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous