

Dynamic Contrast-enhanced and Diffusion-weighted Magnetic Resonance Imaging for Response Evaluation After Single-Dose Ablative Neoadjuvant Partial Breast Irradiation
- PMID: 35387418
- PMCID: PMC8977856
- DOI: 10.1016/j.adro.2021.100854
Dynamic Contrast-enhanced and Diffusion-weighted Magnetic Resonance Imaging for Response Evaluation After Single-Dose Ablative Neoadjuvant Partial Breast Irradiation
Abstract
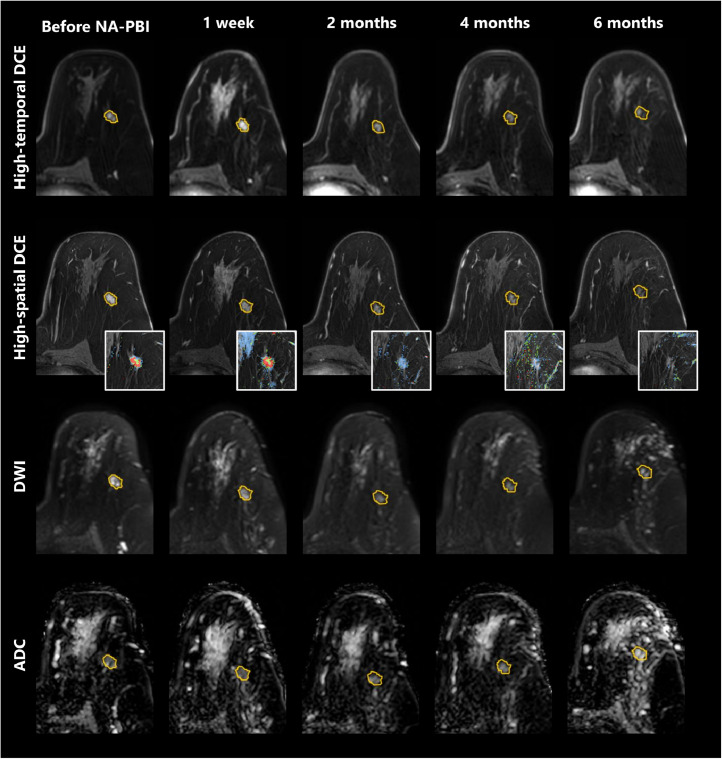
Purpose: We aimed to evaluate changes in dynamic contrast-enhanced (DCE) and diffusion-weighted (DW) magnetic resonance imaging (MRI) scans acquired before and after single-dose ablative neoadjuvant partial breast irradiation (NA-PBI), and explore the relation between semiquantitative MRI parameters and radiologic and pathologic responses.
Methods and materials: We analyzed 3.0T DCE and DW-MRI of 36 patients with low-risk breast cancer who were treated with single-dose NA-PBI, followed by breast-conserving surgery 6 or 8 months later. MRI was acquired before NA-PBI and 1 week, 2, 4, and 6 months after NA-PBI. Breast radiologists assessed the radiologic response and breast pathologists scored the pathologic response after surgery. Patients were grouped as either pathologic responders or nonresponders (<10% vs ≥10% residual tumor cells). The semiquantitative MRI parameters evaluated were time to enhancement (TTE), 1-minute relative enhancement (RE1min), percentage of enhancing voxels (%EV), distribution of washout curve types, and apparent diffusion coefficient (ADC).
Results: In general, the enhancement increased 1 week after NA-PBI (baseline vs 1 week median - TTE: 15s vs 10s; RE1min: 161% vs 197%; %EV: 47% vs 67%) and decreased from 2 months onward (6 months median - TTE: 25s; RE1min: 86%; %EV: 12%). Median ADC increased from 0.83 × 10-3 mm2/s at baseline to 1.28 × 10-3 mm2/s at 6 months. TTE, RE1min, and %EV showed the most potential to differentiate between radiologic responses, and TTE, RE1min, and ADC between pathologic responses.
Conclusions: Semiquantitative analyses of DCE and DW-MRI showed changes in relative enhancement and ADC 1 week after NA-PBI, indicating acute inflammation, followed by changes indicating tumor regression from 2 to 6 months after radiation therapy. A relation between the MRI parameters and radiologic and pathologic responses could not be proven in this exploratory study.
© 2021 The Authors.
Figures



References
-
- Van Der Leij F, Bosma SCJ, Van De Vijver MJ, et al. First results of the preoperative accelerated partial breast irradiation (PAPBI) trial. Radiother Oncol. 2015;114:322–327. - PubMed
-
- Vasmel JE, Charaghvandi RK, Houweling AC, et al. Tumor response following neoadjuvant MR-guided single ablative dose partial breast irradiation. Int J Radiat Oncol. 2020;106:821–829. - PubMed
LinkOut - more resources
Full Text Sources
