

Acute-phase serum amyloid A for early detection of hepatocellular carcinoma in cirrhotic patients with low AFP level
- PMID: 35388082
- PMCID: PMC8986837
- DOI: 10.1038/s41598-022-09713-9
Acute-phase serum amyloid A for early detection of hepatocellular carcinoma in cirrhotic patients with low AFP level
Abstract
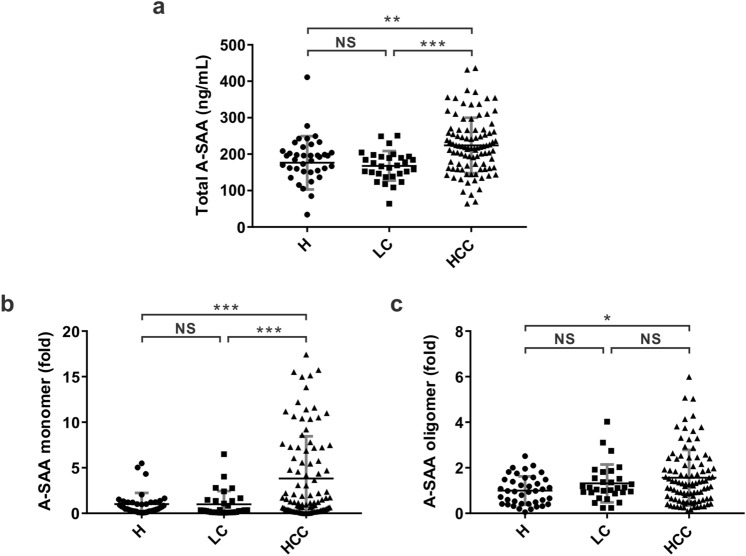
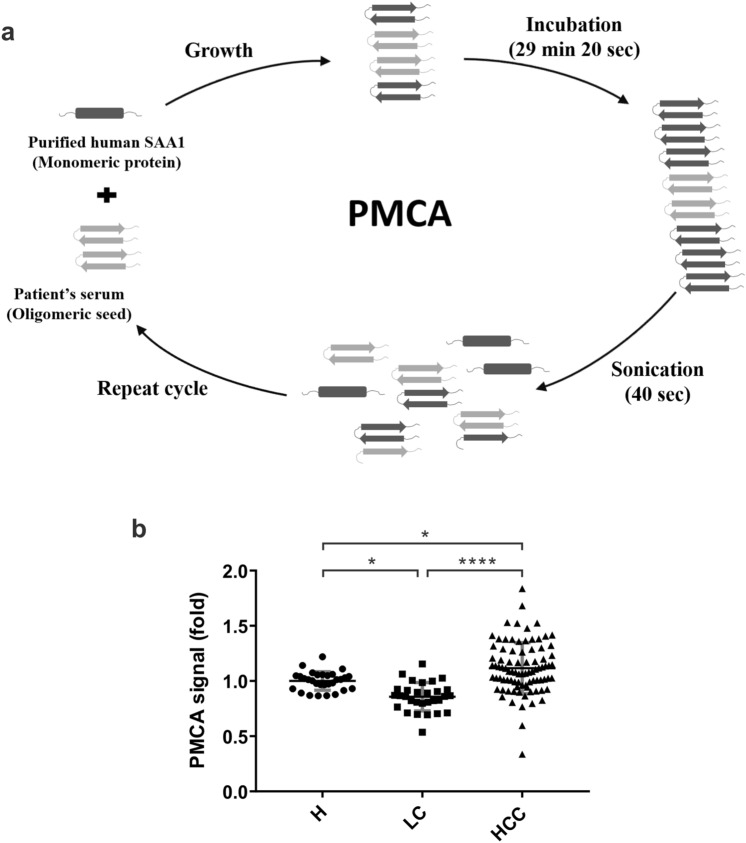
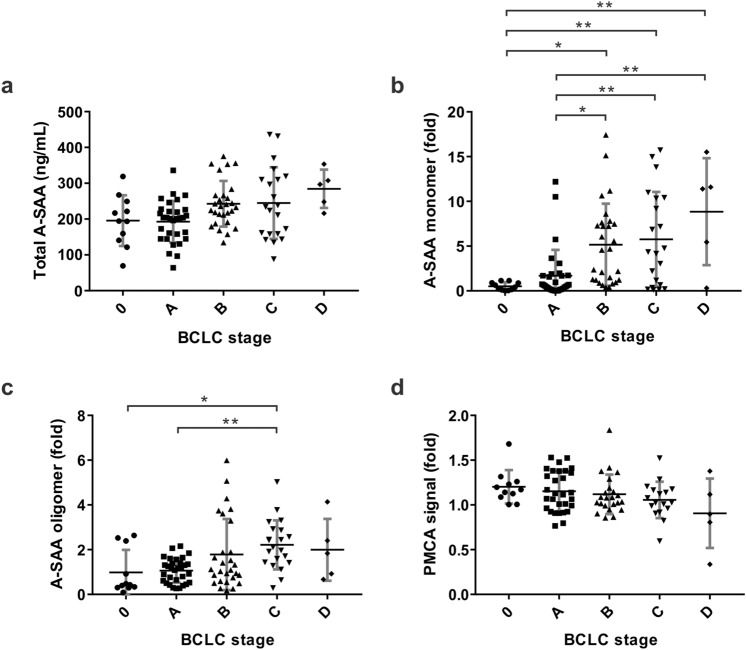
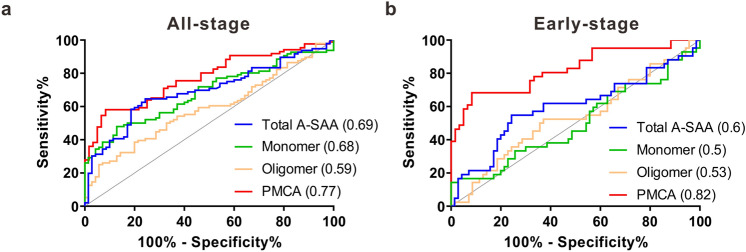
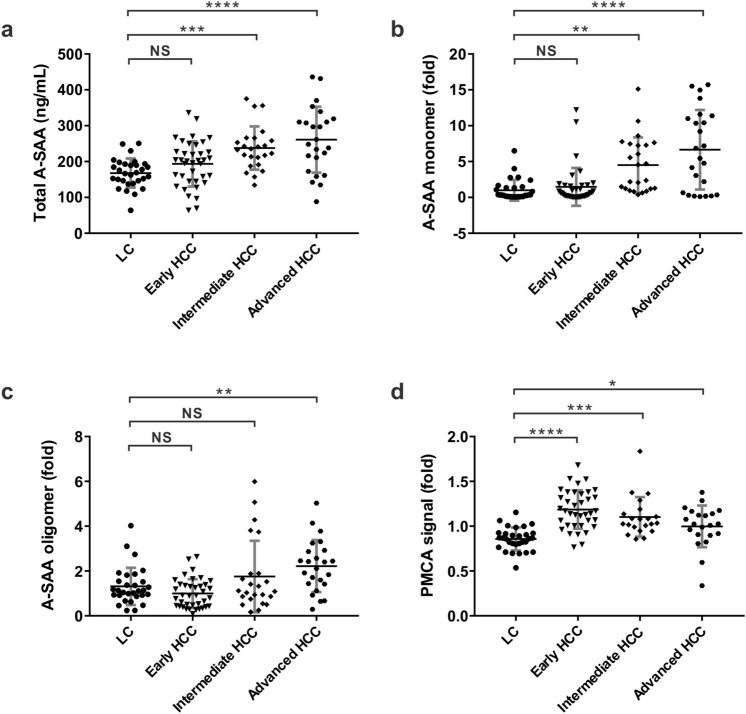
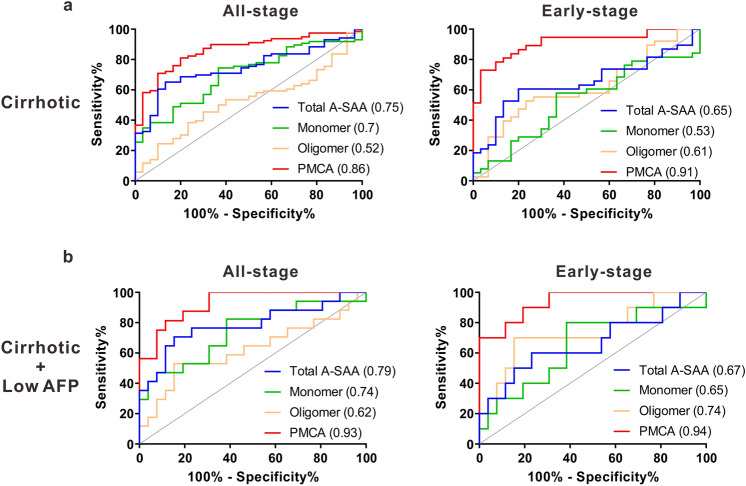
Regular hepatocellular carcinoma (HCC) surveillance by ultrasonography in combination with the α-fetoprotein (AFP) examination is unsatisfactory in diagnostic sensitivity for early-stage HCC especially in cirrhotic patients. We conducted a prospective study in a tertiary medical center in Taiwan and consecutively collected serum samples from patients with chronic hepatitis, liver cirrhosis (LC), or HCC for new biomarker discovery. Overall, 166 patients were enrolled, including 40 hepatitis, 30 LC, and 96 HCC. Four acute-phase serum amyloid A (A-SAA) derived biomarkers including total A-SAA, A-SAA monomer and oligomer, and protein misfolding cyclic amplification (PMCA) signal were measured and compared between patients with and without HCC. A-SAA biomarkers significantly increased in the HCC group when compared to the hepatitis and LC groups, and generally increased in more advanced tumor stages. Among A-SAA biomarkers, the area under the receiver operator characteristic curves (AUROCs) for PMCA signal in discrimination of all-stage and early-stage HCC were 0.86 and 0.9 in cirrhotic patients, which is comparable to AFP. For cirrhotic patients with low AFP (< 7 ng/mL), PMCA signal maintained good capacity in prediction of early-stage HCC (AUROC: 0.94). Serum A-SAA and its prion-like property showed a potential to complement AFP in detection of early-stage HCC.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
[Clinical value of plasma scaffold protein SEC16A in evaluating hepatitis B-related liver cirrhosis and hepatocellular carcinoma].Zhonghua Gan Zang Bing Za Zhi. 2023 Jun 20;31(6):621-626. doi: 10.3760/cma.j.cn501113-20230220-00067. Zhonghua Gan Zang Bing Za Zhi. 2023. PMID: 37400387 Chinese.
-
Combined use of AFP, PIVKA-II, and AFP-L3 as tumor markers enhances diagnostic accuracy for hepatocellular carcinoma in cirrhotic patients.Scand J Gastroenterol. 2016 Mar;51(3):344-53. doi: 10.3109/00365521.2015.1082190. Epub 2015 Sep 4. Scand J Gastroenterol. 2016. PMID: 26340708
-
The Expressions of CD44, CD90 and Alpha Fetoprotein Biomarkers in Indonesian Patients with Advanced Liver Disease: an Observational Study.Acta Med Indones. 2019 Apr;51(2):137-144. Acta Med Indones. 2019. PMID: 31383828
-
Blood-based biomarkers for hepatocellular carcinoma screening: Approaching the end of the ultrasound era?J Hepatol. 2023 Jan;78(1):207-216. doi: 10.1016/j.jhep.2022.08.036. Epub 2022 Sep 8. J Hepatol. 2023. PMID: 36089157 Free PMC article. Review.
-
Surveillance of hepatocellular carcinoma in cirrhotic patients: Current knowledge and future directions.Hepatol Forum. 2020 Sep 21;1(3):112-118. doi: 10.14744/hf.2020.2020.0003. eCollection 2020 Sep. Hepatol Forum. 2020. PMID: 35949723 Free PMC article. Review.
Cited by
-
Early life exposure to vitamin D deficiency impairs molecular mechanisms that regulate liver cholesterol biosynthesis, energy metabolism, inflammation, and detoxification.Front Endocrinol (Lausanne). 2024 May 10;15:1335855. doi: 10.3389/fendo.2024.1335855. eCollection 2024. Front Endocrinol (Lausanne). 2024. PMID: 38800476 Free PMC article.
-
Differential Protease Specificity by Collagenase as a Novel Approach to Serum Proteomics That Includes Identification of Extracellular Matrix Proteins without Enrichment.J Am Soc Mass Spectrom. 2024 Mar 6;35(3):487-497. doi: 10.1021/jasms.3c00366. Epub 2024 Feb 8. J Am Soc Mass Spectrom. 2024. PMID: 38329320 Free PMC article.
-
Serum amyloid alpha 1-2 are not required for liver inflammation in the 4T1 murine breast cancer model.Front Immunol. 2023 Feb 3;14:1097788. doi: 10.3389/fimmu.2023.1097788. eCollection 2023. Front Immunol. 2023. PMID: 36817472 Free PMC article.
-
New insights into potential biomarkers and their roles in biological processes associated with hepatitis C-related liver cirrhosis by hepatic RNA-seq-based transcriptome profiling.Virus Res. 2024 Nov;349:199457. doi: 10.1016/j.virusres.2024.199457. Epub 2024 Sep 10. Virus Res. 2024. PMID: 39216827 Free PMC article.
-
Function of the Long Noncoding RNAs in Hepatocellular Carcinoma: Classification, Molecular Mechanisms, and Significant Therapeutic Potentials.Bioengineering (Basel). 2022 Aug 21;9(8):406. doi: 10.3390/bioengineering9080406. Bioengineering (Basel). 2022. PMID: 36004931 Free PMC article. Review.
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
