

Intraoperative MET-receptor targeted fluorescent imaging and spectroscopy for lymph node detection in papillary thyroid cancer: novel diagnostic tools for more selective central lymph node compartment dissection
- PMID: 35389070
- PMCID: PMC9308606
- DOI: 10.1007/s00259-022-05763-3
Intraoperative MET-receptor targeted fluorescent imaging and spectroscopy for lymph node detection in papillary thyroid cancer: novel diagnostic tools for more selective central lymph node compartment dissection
Abstract
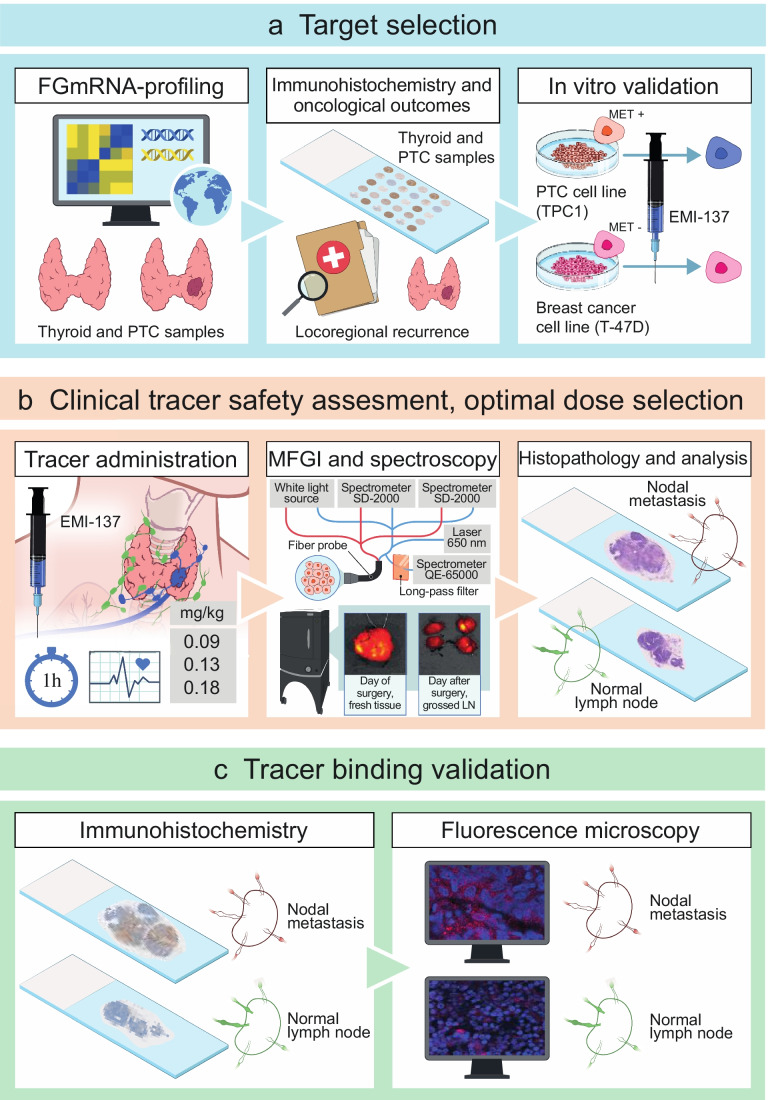
Purpose: Patients undergoing prophylactic central compartment dissection (PCLND) for papillary thyroid cancer (PTC) are often overtreated. This study aimed to determine if molecular fluorescence-guided imaging (MFGI) and spectroscopy can be useful for detecting PTC nodal metastases (NM) and to identify negative central compartments intraoperatively.
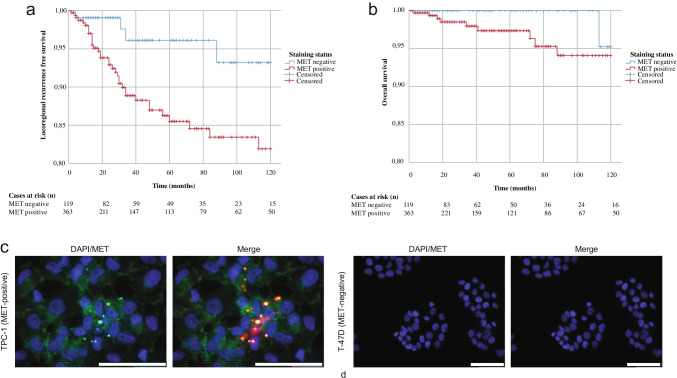
Methods: We used a data-driven prioritization strategy based on transcriptomic profiles of 97 primary PTCs and 80 normal thyroid tissues (NTT) to identify tumor-specific antigens for a clinically available near-infrared fluorescent tracer. Protein expression of the top prioritized antigen was immunohistochemically validated with a tissue microarray containing primary PTC (n = 741) and NTT (n = 108). Staining intensity was correlated with 10-year locoregional recurrence-free survival (LRFS). A phase 1 study (NCT03470259) with EMI-137, targeting MET, was conducted to evaluate safety, optimal dosage for detecting PTC NM with MFGI, feasibility of NM detection with quantitative fiber-optic spectroscopy, and selective binding of EMI-137 for MET.
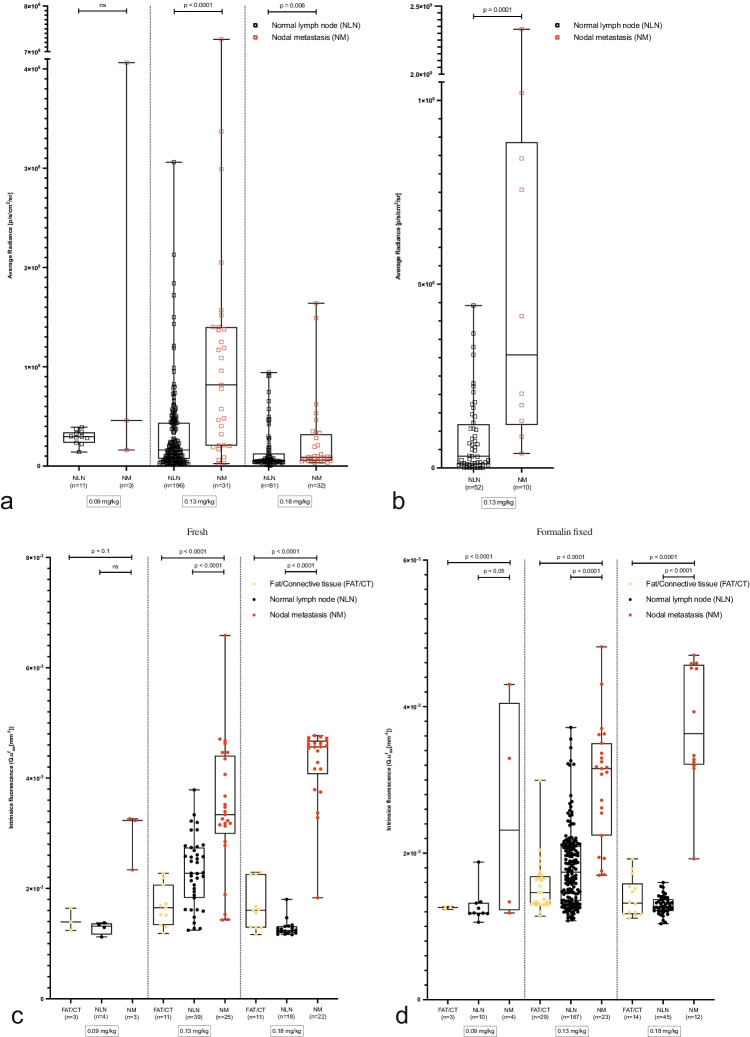
Results: MET was selected as the most promising antigen. A worse LRFS was observed in patients with positive versus negative MET staining (81.9% versus 93.2%; p = 0.02). In 19 patients, no adverse events related to EMI-137 occurred. 0.13 mg/kg EMI-137 was selected as optimal dosage for differentiating NM from normal lymph nodes using MFGI (p < 0.0001) and spectroscopy (p < 0.0001). MFGI identified 5/19 levels (26.3%) without NM. EMI-137 binds selectively to MET.
Conclusion: MET is overexpressed in PTC and associated with increased locoregional recurrence rates. Perioperative administration of EMI-137 is safe and facilitates NM detection using MFGI and spectroscopy, potentially reducing the number of negative PCLNDs with more than 25%.
Clinical trial registration: NCT03470259.
Keywords: Lymph node imaging; Molecular fluorescence-guided imaging; Papillary thyroid cancer; Spectroscopy.
© 2022. The Author(s).
Conflict of interest statement
GMvD is a member of the scientific board of SurgVision BV, founder, shareholder, and CEO of TRACER Europe BV (Groningen, the Netherlands). None of the other authors reported any potential conflicts of interest.
Figures

References
-
- Haugen BR, et al. 2015 American Thyroid Association management guidelines for adult patients with thyroid nodules and differentiated thyroid cancer: the American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer. Thyroid : official journal of the American Thyroid Association. 2016;26:1–133. doi: 10.1089/thy.2015.0020. - DOI - PMC - PubMed
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
