

Consensus Obtained for the Nephrotoxic Potential of 167 Drugs in Adult Critically Ill Patients Using a Modified Delphi Method
- PMID: 35389144
- PMCID: PMC8988110
- DOI: 10.1007/s40264-022-01173-4
Consensus Obtained for the Nephrotoxic Potential of 167 Drugs in Adult Critically Ill Patients Using a Modified Delphi Method
Abstract
Introduction: The approach to evaluating nephrotoxins in studies of drug-associated acute kidney injury varies. Some studies use a list of under ten drugs for evaluation whereas others include over 100 drugs. Drugs are typically assigned a binary classification, nephrotoxic or not nephrotoxic. This oversimplifies the nephrotoxic potential of the drugs under investigation.
Objective: This study aimed to assign a nephrotoxin potential for 167 drugs used in the adult critical care setting.
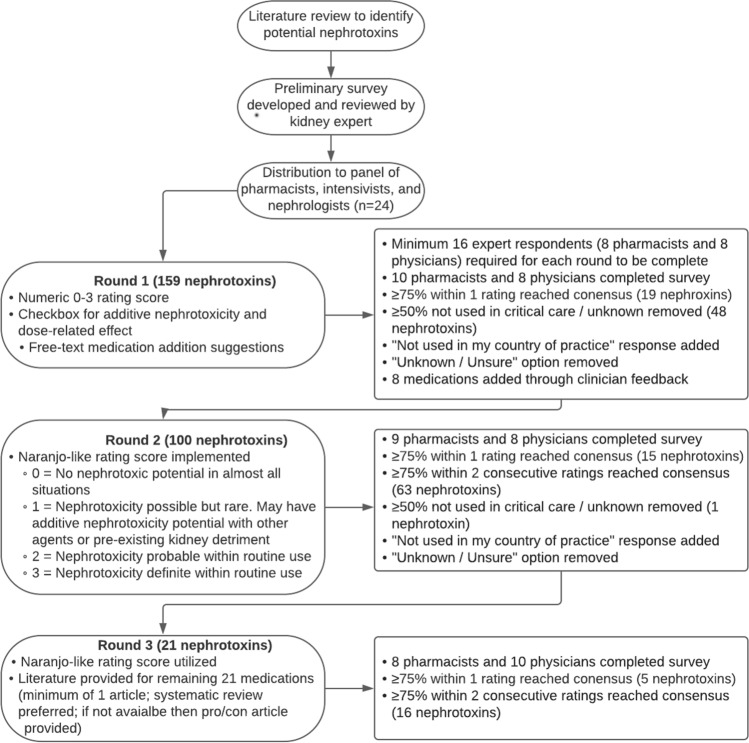
Methods: A three-round, international, interdisciplinary, web-based modified-Delphi study was used to evaluate nephrotoxins used in adult critically ill patients. Twenty-four international experienced clinicians were identified through the Acute Disease Quality Initiative group and professional affiliations. Included individuals represented the fields of intensive care, nephrology, and pharmacy. One hundred and fifty-nine medications were identified from the literature, with eight additional medications added after the first round, for a total of 167 medications. The primary outcome was consensus achieved for nephrotoxicity ratings. Scores were evaluated each round to determine if a consensus was met.
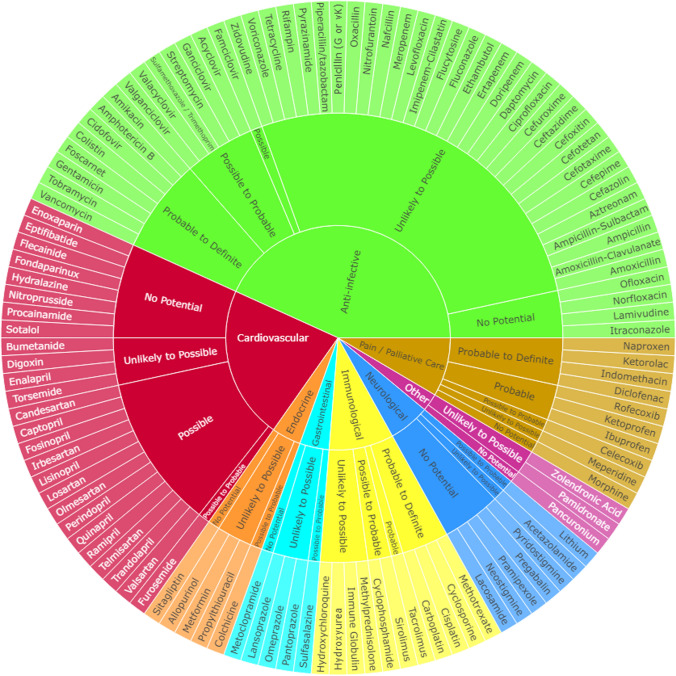
Results: Our nephrotoxin potential index rating indicated that 20 drugs were nephrotoxicity probable or probable/definite per consensus. Nephrotoxic potential was assessed based on the standard use of medications in intensive care and the following consensus scores: 0 = no nephrotoxic potential, 1 = possible nephrotoxic potential, 2 = probable nephrotoxic potential, 3 = definite nephrotoxic potential.
Conclusions: The nephrotoxin potential index rating allows for prioritization of targeted drugs with greater nephrotoxic potential for institutional nephrotoxin stewardship programs. Furthermore, the nephrotoxin potential index rating provides homogeneity for research and guidance on detailed assessments by severity for each drug.
© 2022. The Author(s), under exclusive licence to Springer Nature Switzerland AG.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
