

Skeletal Muscle Disorders: A Noncardiac Source of Cardiac Troponin T
- PMID: 35389756
- PMCID: PMC10069758
- DOI: 10.1161/CIRCULATIONAHA.121.058489
Skeletal Muscle Disorders: A Noncardiac Source of Cardiac Troponin T
Abstract
Background: Cardiac troponin (cTn) T and cTnI are considered cardiac specific and equivalent in the diagnosis of acute myocardial infarction. Previous studies suggested rare skeletal myopathies as a noncardiac source of cTnT. We aimed to confirm the reliability/cardiac specificity of cTnT in patients with various skeletal muscle disorders (SMDs).
Methods: We prospectively enrolled patients presenting with muscular complaints (≥2 weeks) for elective evaluation in 4 hospitals in 2 countries. After a cardiac workup, patients were adjudicated into 3 predefined cardiac disease categories. Concentrations of cTnT/I and resulting cTnT/I mismatches were assessed with high-sensitivity (hs-) cTnT (hs-cTnT-Elecsys) and 3 hs-cTnI assays (hs-cTnI-Architect, hs-cTnI-Access, hs-cTnI-Vista) and compared with those of control subjects without SMD presenting with adjudicated noncardiac chest pain to the emergency department (n=3508; mean age, 55 years; 37% female). In patients with available skeletal muscle biopsies, TNNT/I1-3 mRNA differential gene expression was compared with biopsies obtained in control subjects without SMD.
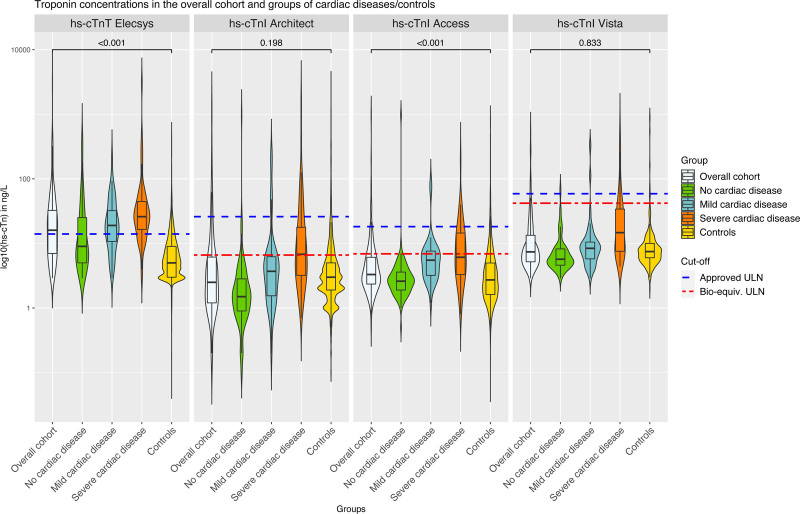
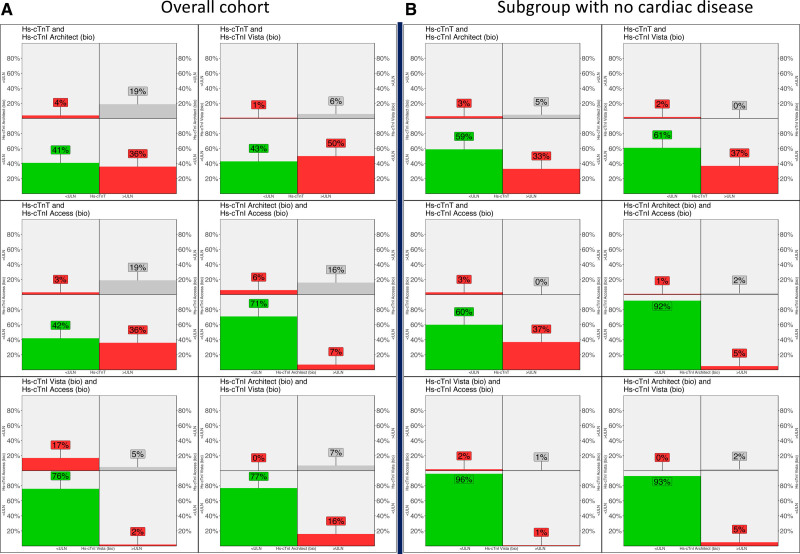
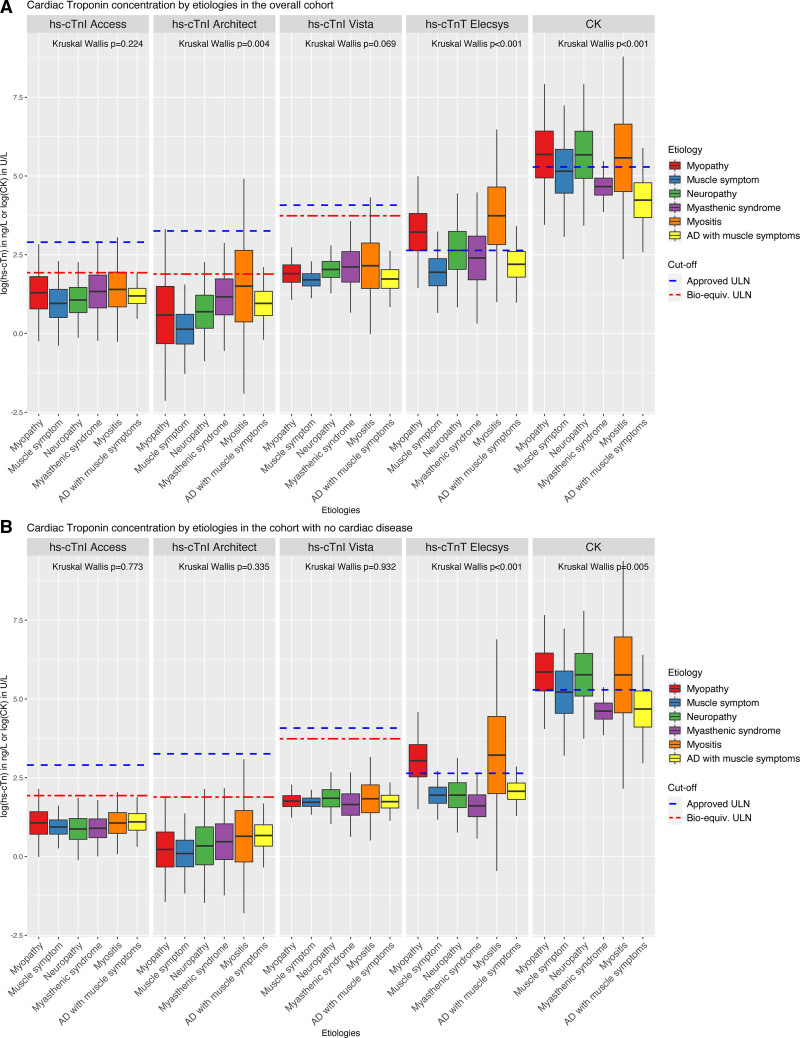
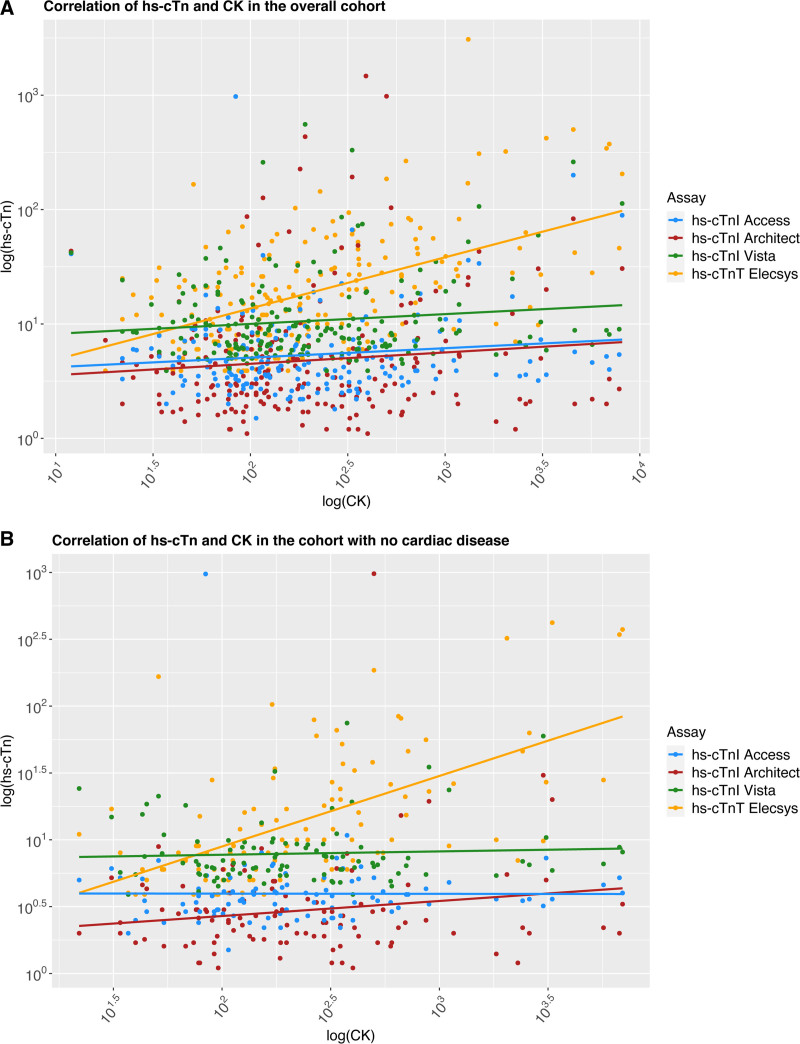
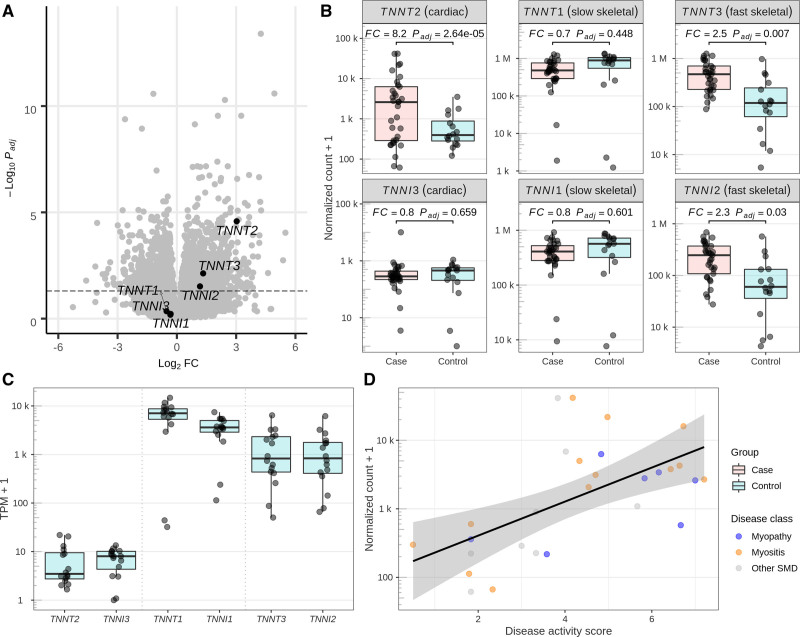
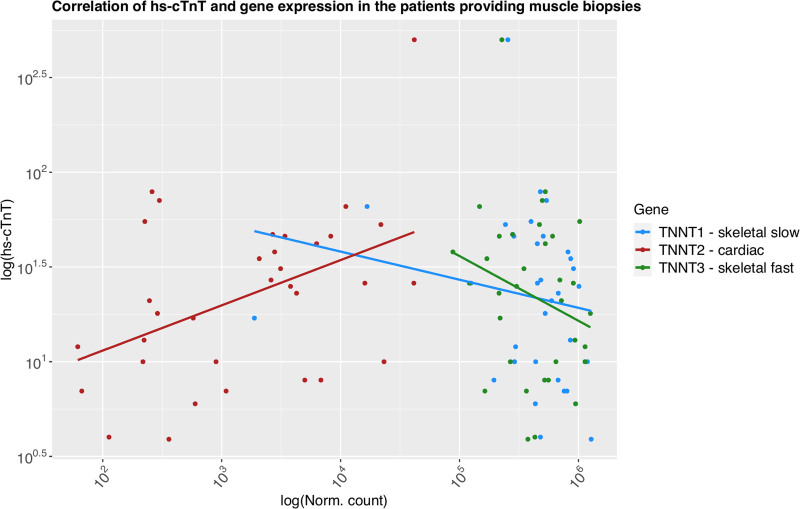
Results: Among 211 patients (mean age, 57 years; 42% female), 108 (51%) were adjudicated to having no cardiac disease, 44 (21%) to having mild disease, and 59 (28%) to having severe cardiac disease. hs-cTnT/I concentrations significantly increased from patients with no to those with mild and severe cardiac disease for all assays (all P<0.001). hs-cTnT-Elecsys concentrations were significantly higher in patients with SMD versus control subjects (median, 16 ng/L [interquartile range (IQR), 7-32.5 ng/L] versus 5 ng/L [IQR, 3-9 ng/L]; P<0.001), whereas hs-cTnI concentrations were mostly similar (hs-cTnI-Architect, 2.5 ng/L [IQR, 1.2-6.2 ng/L] versus 2.9 ng/L [IQR, 1.8-5.0 ng/L]; hs-cTnI-Access, 3.3 ng/L [IQR, 2.4-6.1 ng/L] versus 2.7 ng/L [IQR, 1.6-5.0 ng/L]; and hs-cTnI-Vista, 7.4 ng/L [IQR, 5.2-13.4 ng/L] versus 7.5 ng/L [IQR, 6-10 ng/L]). hs-cTnT-Elecsys concentrations were above the upper limit of normal in 55% of patients with SMD versus 13% of control subjects (P<0.01). mRNA analyses in skeletal muscle biopsies (n=33), mostly (n=24) from individuals with noninflammatory myopathy and myositis, showed 8-fold upregulation of TNNT2, encoding cTnT (but none for TNNI3, encoding cTnI) versus control subjects (n=16, PWald<0.001); the expression correlated with pathological disease activity (R=0.59, Pt-statistic<0.001) and circulating hs-cTnT concentrations (R=0.26, Pt-statistic=0.031).
Conclusions: In patients with active chronic SMD, elevations in cTnT concentrations are common and not attributable to cardiac disease in the majority. This was not observed for cTnI and may be explained in part by re-expression of cTnT in skeletal muscle.
Registration: URL: https://www.
Clinicaltrials: gov; Unique identifier: NCT03660969.
Keywords: muscle, skeletal; myocardial infarction; myopathies, structural, congenital; troponin.
Conflict of interest statement
Dr Jeanne du Fay de Lavallaz has received research support from the Swiss Heart Foundation. Dr Nestelberger has received research support from the Swiss National Science Foundation (P400PM_191037/1), the Prof Dr Max Cloëtta Foundation, the Margarete und Walter Lichtenstein-Stiftung (3MS1038), and the University Hospital Basel, as well as speaker honoraria/consulting honoraria from Siemens, Beckman Coulter, Bayer, Ortho Clinical Diagnostics, and Orion Pharma, outside the submitted work. Dr Boeddinghaus has received research grants from the University of Basel and the Division of Internal Medicine, the Swiss Academy of Medical Sciences, and the Gottfried and Julia Bangerter-Rhyner-Foundation, and speaker honoraria from Siemens, Roche, Ortho Clinical Diagnostics, and Quidel Corp, outside the submitted work. Dr Mueller has received research support from the Swiss National Science Foundation, the Swiss Heart Foundation, the KTI, the University Hospital Basel, the University of Basel, Abbott, Beckman Coulter, Idorsia, Novartis, Ortho Clinical Diagnostics, Quidel, Roche, and Siemens, as well as speaker honoraria/consulting honoraria from Amgen, AstraZeneca, Bayer, Boehringer Ingelheim, BMS, Daiichi Sankyo, Idorsia, Novartis, Osler, Roche, and Sanofi, outside the submitted work. Dr Maurer has grant/research support from the Prof Max Cloetta Foundation, AbbVie, Protagen, and Novartis Biomedical Research and received speaker fees from Boehringer-Ingelheim, as well as congress support from Pfizer, Roche, Actelion, Mepha, and MSD. In addition, Dr. Maurer has a patent mir-29 for the treatment of systemic sclerosis issued (US8247389, EP2331143), all outside the submitted work. Dr Gualandro received research grants from Fundacao de Amparo a Pesquisa do Estado de Sao Paulo, Brasil and consulting honoraria from Roche, outside the submitted work. Dr Lopez-Ayala has received research support from the Swiss Heart Foundation (FF20079). Dr Puelacher reports research funding from Roche Diagnostics, the University of Basel, and the University Hospital Basel, outside of the submitted work. Dr Sinnreich has received financial support from Roche from 2015 to 2019 for a research collaboration unrelated to the current work. The other authors report no conflicts. The hs-cTn assays investigated were donated by the manufacturers, who had no role in the design of the study, the analysis of the data, the preparation of the manuscript, or the decision to submit the manuscript for publication.
Figures
Comment in
-
At the Crossroad Between Skeletal and Cardiac Muscle Cells.Circulation. 2022 Jun 14;145(24):1780-1783. doi: 10.1161/CIRCULATIONAHA.122.059935. Epub 2022 Jun 13. Circulation. 2022. PMID: 35696457 Free PMC article. No abstract available.
-
Response by du Fay de Lavallaz et al to Letter Regarding Article, "Skeletal Muscle Disorders: A Noncardiac Source of Cardiac Troponin T".Circulation. 2022 Oct 11;146(15):e204. doi: 10.1161/CIRCULATIONAHA.122.061976. Epub 2022 Oct 10. Circulation. 2022. PMID: 36214135 No abstract available.
-
Letter by Giannitsis et al Regarding Article, "Skeletal Muscle Disorders: A Noncardiac Source of Cardiac Troponin T".Circulation. 2022 Oct 11;146(15):e202-e203. doi: 10.1161/CIRCULATIONAHA.122.060812. Epub 2022 Oct 10. Circulation. 2022. PMID: 36214136 No abstract available.
References
-
- Gomes AV, Potter JD, Szczesna-Cordary D. The role of troponins in muscle contraction. IUBMB Life. 2002;54:323–333. doi: 10.1080/15216540216037 - PubMed
-
- Gordon AM, Homsher E, Regnier M. Regulation of contraction in striated muscle. Physiol Rev. 2000;80:853–924. doi: 10.1152/physrev.2000.80.2.853 - PubMed
-
- Thygesen K, Alpert JS, Jaffe AS, Chaitman BR, Bax JJ, Morrow DA, White HD; Executive Group on behalf of the Joint European Society of Cardiology (ESC)/American College of Cardiology (ACC)/American Heart Association (AHA)/World Heart Federation (WHF) Task Force for the Universal Definition of Myocardial Infarction. Fourth universal definition of myocardial infarction (2018). Circulation. 2018;138:e618–e651. doi: 10.1161/CIR.0000000000000617 - PubMed
-
- Neumann JT, Twerenbold R, Ojeda F, Sörensen NA, Chapman AR, Shah ASV, Anand A, Boeddinghaus J, Nestelberger T, Badertscher P, et al. . Application of high-sensitivity troponin in suspected myocardial infarction. N Engl J Med. 2019;380:2529–2540. doi: 10.1056/NEJMoa1803377 - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
