

Comprehensive cancer-oriented biobanking resource of human samples for studies of post-zygotic genetic variation involved in cancer predisposition
- PMID: 35390022
- PMCID: PMC8989288
- DOI: 10.1371/journal.pone.0266111
Comprehensive cancer-oriented biobanking resource of human samples for studies of post-zygotic genetic variation involved in cancer predisposition
Abstract
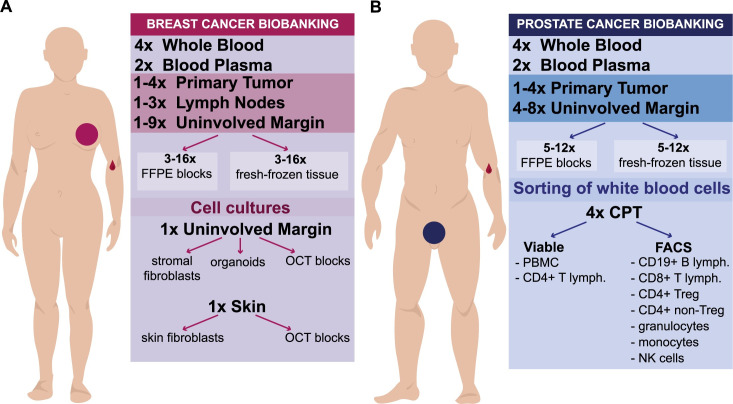
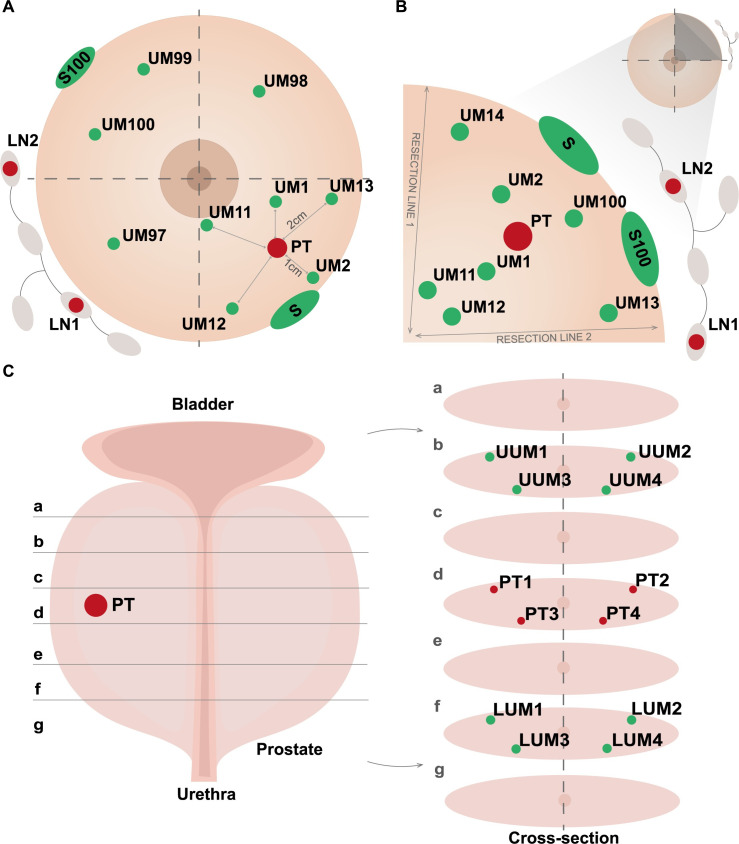
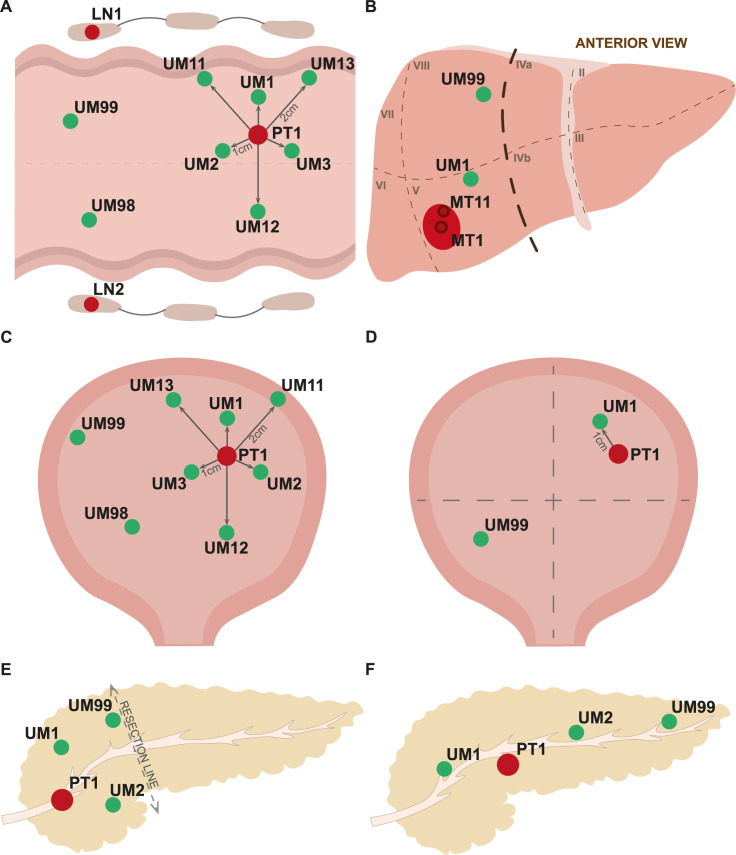
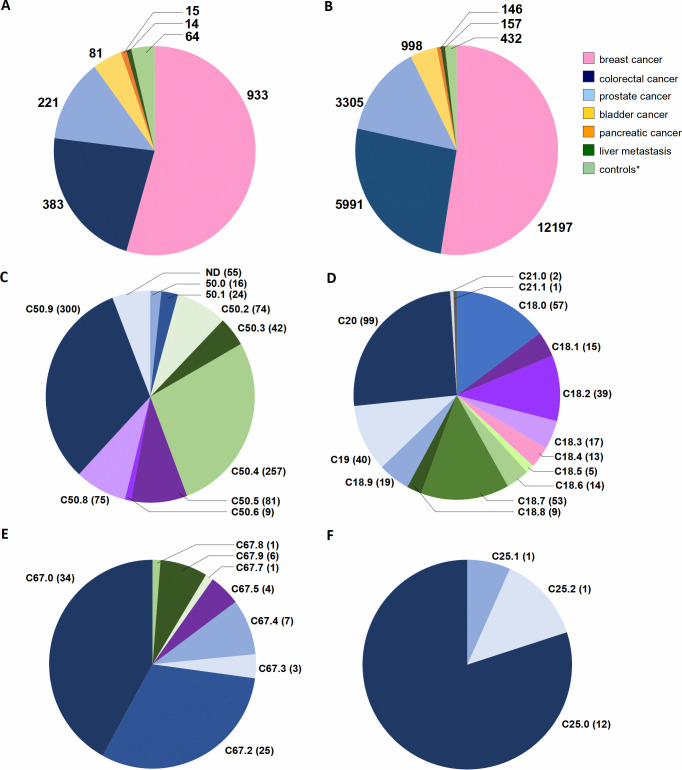
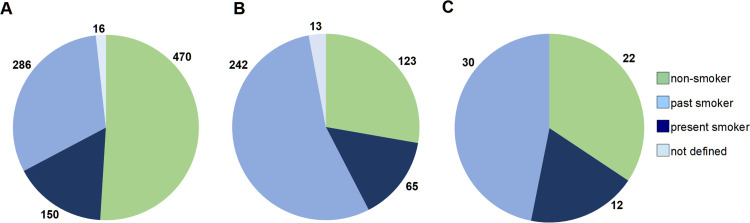
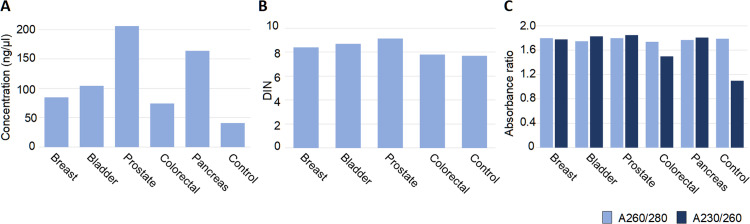
The progress in translational cancer research relies on access to well-characterized samples from a representative number of patients and controls. The rationale behind our biobanking are explorations of post-zygotic pathogenic gene variants, especially in non-tumoral tissue, which might predispose to cancers. The targeted diagnoses are carcinomas of the breast (via mastectomy or breast conserving surgery), colon and rectum, prostate, and urinary bladder (via cystectomy or transurethral resection), exocrine pancreatic carcinoma as well as metastases of colorectal cancer to the liver. The choice was based on the high incidence of these cancers and/or frequent fatal outcome. We also collect age-matched normal controls. Our still ongoing collection originates from five clinical centers and after nearly 2-year cooperation reached 1711 patients and controls, yielding a total of 23226 independent samples, with an average of 74 donors and 1010 samples collected per month. The predominant diagnosis is breast carcinoma, with 933 donors, followed by colorectal carcinoma (383 donors), prostate carcinoma (221 donors), bladder carcinoma (81 donors), exocrine pancreatic carcinoma (15 donors) and metachronous colorectal cancer metastases to liver (14 donors). Forty percent of the total sample count originates from macroscopically healthy cancer-neighboring tissue, while contribution from tumors is 12%, which adds to the uniqueness of our collection for cancer predisposition studies. Moreover, we developed two program packages, enabling registration of patients, clinical data and samples at the participating hospitals as well as the central system of sample/data management at coordinating center. The approach used by us may serve as a model for dispersed biobanking from multiple satellite hospitals. Our biobanking resource ought to stimulate research into genetic mechanisms underlying the development of common cancers. It will allow all available "-omics" approaches on DNA-, RNA-, protein- and tissue levels to be applied. The collected samples can be made available to other research groups.
Conflict of interest statement
J.P.D. is cofounder and shareholder in Cray Innovation AB. The remaining authors have declared that no competing interests exist.
Figures
References
-
- Ronowicz A, Janaszak-Jasiecka A, Skokowski J, Madanecki P, Bartoszewski R, Balut M, et al.. Concurrent DNA Copy-Number Alterations and Mutations in Genes Related to Maintenance of Genome Stability in Uninvolved Mammary Glandular Tissue from Breast Cancer Patients. Hum Mutat. 2015;36(11):1088–99. Epub 2015/07/30. doi: 10.1002/humu.22845 . - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
