

Intestinal Damage in COVID-19: SARS-CoV-2 Infection and Intestinal Thrombosis
- PMID: 35391725
- PMCID: PMC8981312
- DOI: 10.3389/fmicb.2022.860931
Intestinal Damage in COVID-19: SARS-CoV-2 Infection and Intestinal Thrombosis
Abstract
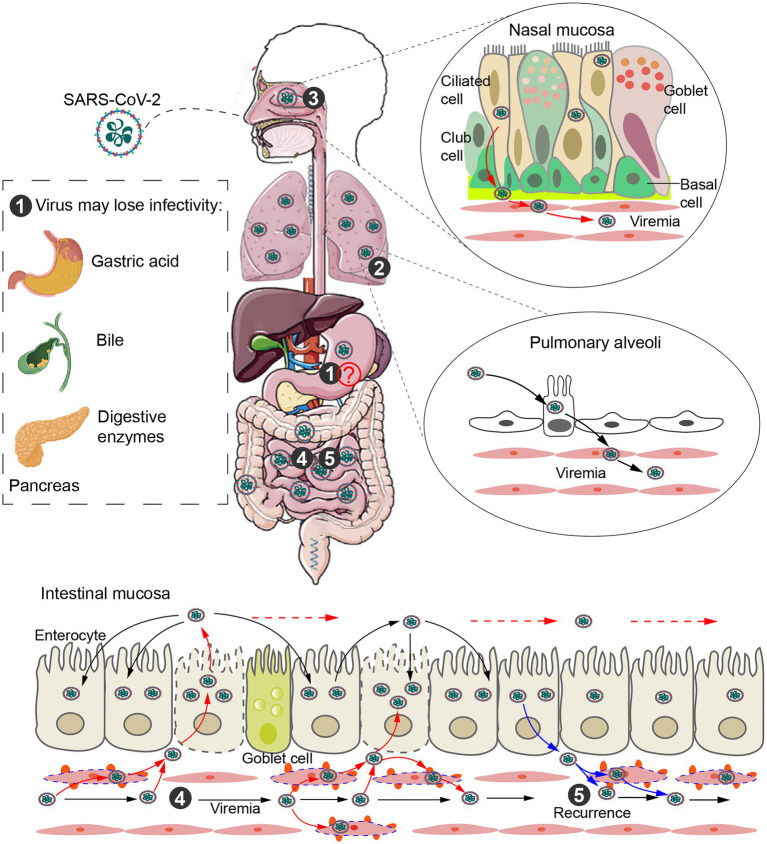
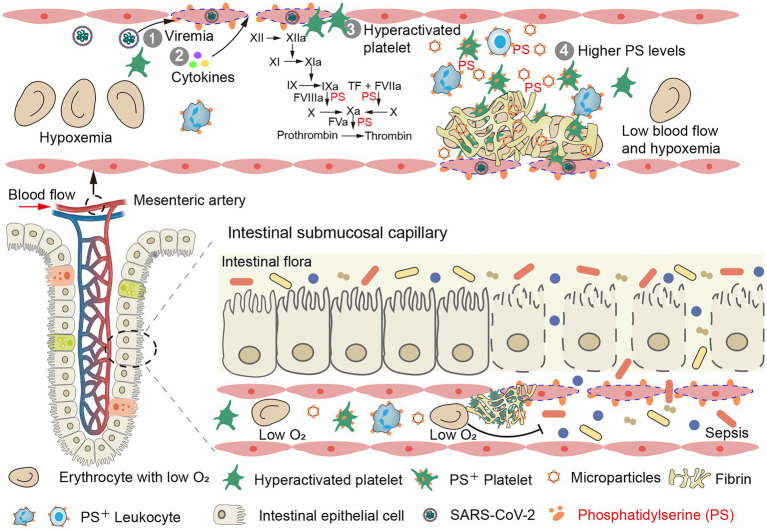
The intestinal tract, with high expression of angiotensin-converting enzyme 2 (ACE2), is a major site of extrapulmonary infection in COVID-19. During pulmonary infection, the virus enters the bloodstream forming viremia, which infects and damages extrapulmonary organs. Uncontrolled viral infection induces cytokine storm and promotes a hypercoagulable state, leading to systemic microthrombi. Both viral infection and microthrombi can damage the gut-blood barrier, resulting in malabsorption, malnutrition, and intestinal flora entering the blood, ultimately increasing disease severity and mortality. Early prophylactic antithrombotic therapy can prevent these damages, thereby reducing mortality. In this review, we discuss the effects of SARS-CoV-2 infection and intestinal thrombosis on intestinal injury and disease severity, as well as corresponding treatment strategies.
Keywords: COVID-19; antithrombotic therapy; blood transmission; intestinal infection; intestinal thrombosis.
Copyright © 2022 Wu, Jing, Wang, Wang, Zuo, Jiang, Novakovic and Shi.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest. The reviewer (UDA) declared a shared affiliation with the authors (VN and JS) to the handling editor at the time of review.
Figures
References
-
- Ananworanich J., Mogg R., Dunne M. W., Bassyouni M., David C. V., Gonzalez E., et al. . (2021). Randomized study of rivaroxaban vs. placebo on disease progression and symptoms resolution in high-risk adults with mild COVID-19. Clin. Infect. Dis. doi: 10.1093/cid/ciab813, PMID: [Epub ahead of print]. - DOI - PMC - PubMed
-
- Antonelli M., Penfold R. S., Merino J., Sudre C. H., Molteni E., Berry S., et al. . (2022). Risk factors and disease profile of post-vaccination SARS-CoV-2 infection in UK users of the COVID symptom study app: a prospective, community-based, nested, case-control study. Lancet Infect. Dis. 22, 43–55. doi: 10.1016/S1473-3099(21)00460-6 - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous