

"Slim-Mesh" Technique for Giant Ventral Hernia
- PMID: 35391780
- PMCID: PMC8983121
- DOI: 10.4293/JSLS.2021.00079
"Slim-Mesh" Technique for Giant Ventral Hernia
Abstract
Background and objective: We devised a sutureless "Slim-Mesh" technique to treat ventral hernias, including large-giant/massive ones, reduce intra- and postoperative complications, and lower operation time.
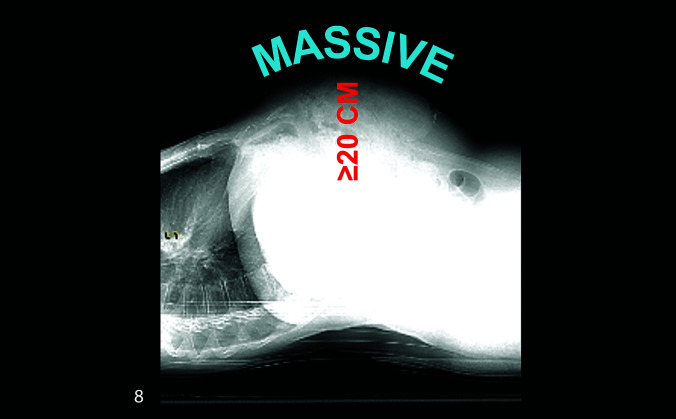
Methods: Between September 1, 2009 and October 31, 2020, 43 patients with large (10 - 14.9 cm)-giant (15 - 19.9 cm) and massive (≥ 20 cm) ventral hernia were operated at our Department with the above technique. This was a prospective (79%)-retrospective study.
Results: This study comprised 22 males and 21 females. Mean age was 63 years. Large-giant and massive hernias were found intraoperatively in 37 and 6 cases respectively. Mean operation time for all hernias was 116 minutes, 104 for large-giant hernias, and 190 for massive. In 53.4% of cases, hernia-neck operative measurement was larger than preoperative size. In 25.5% of cases, laparoscopy found satellite hernias previously undetected by ultrasound- and/or computed tomography scan. A composite mesh and a noncomposite mesh were used in 95% and 5% of cases respectively. For mesh fixation, titanium tacks and absorbable straps were used in 14% and 86% of cases respectively. Mean length of hospital stay was 2.3 days. Mean follow-up time was 3 years and 4 months. In our study, there were 5 early postoperative complications: 3 seromas, 1 trocar-site hernia, and 1 case of cystitis. We found 2 late small symptomless recurrences (4.6%).
Conclusion: The sutureless "Slim-Mesh" technique facilitates intra-abdominal introduction, as well as the handling and fixation of giant and monster (36 × 26 cm) meshes. In our experience, "Slim-Mesh" is safe, simple, and fast, and economical even for large-giant/massive ventral hernia repair.
Keywords: Giant ventral hernia repair; Massive ventral hernia; Operation time; Postoperative pain; Slim-Mesh technique.
© 2022 by SLS, Society of Laparoscopic & Robotic Surgeons.
Conflict of interest statement
Conflict of interests: none.
Figures








References
-
- Helgstrand F. National results after ventral hernia repair. Dan Med J. 2016;63(7):Pii: B5258. - PubMed
-
- Bikhchandani J, Fitzgibbons RJ. Jr. Repair of giant ventral hernias. Adv Surg. 2013;47:1–27. - PubMed
-
- Memon AA, Khan A, Zafar H, Murtaza G, Zaidi M. Repair of large and giant incisional hernia with onlay mesh: perspective of a tertiary care hospital of a developing country. Int J Surg. 2013;11(1):41–45. - PubMed
-
- Passot G, Villeneuve L, Sabbagh C, et al. . Fédération de Recherche en Chirurgie (FRENCH). Definition of giant ventral hernias: development of standardization through a practice survey. Int J Surg. 2016;28:136–140. Epub 2016 Feb. - PubMed
-
- Korenkov M, Paul A, Sauerland S, et al. . Classification and surgical treatment of incisional hernia. Results of an experts' meeting. Langenbecks Arch Surg. 2001;386(1):65–73. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials