

Four-level anterior versus posterior cervical fusions: Perioperative outcomes and five-year reoperation rates: Outcomes after four-level anterior versus posterior cervical procedures
- PMID: 35392022
- PMCID: PMC8980614
- DOI: 10.1016/j.xnsj.2022.100115
Four-level anterior versus posterior cervical fusions: Perioperative outcomes and five-year reoperation rates: Outcomes after four-level anterior versus posterior cervical procedures
Abstract
Background: Multilevel cervical pathology can often be addressed via anterior cervical discectomy and fusion (ACDF) or posterior cervical fusion (PCF). While posterior procedures may be technically easier for four-level pathology, there are advantages and disadvantages to both approaches that make it of interest to compare outcomes. The purpose was to compare perioperative adverse events and long-term cervical reoperation rates of four-level ACDF and PCF.
Methods: The 2010 to Q1 2020 PearlDiver MSpine database was queried. Patients undergoing isolated elective four-level ACDF or PCF were identified (excluding cases performed for trauma, neoplasm, and/or infections) and 1:1 matched based on age, sex, and comorbidities. Ninety-day adverse events were compared with univariate and multivariate analyses. Five-year incidences of subsequent cervical reoperations were also compared.
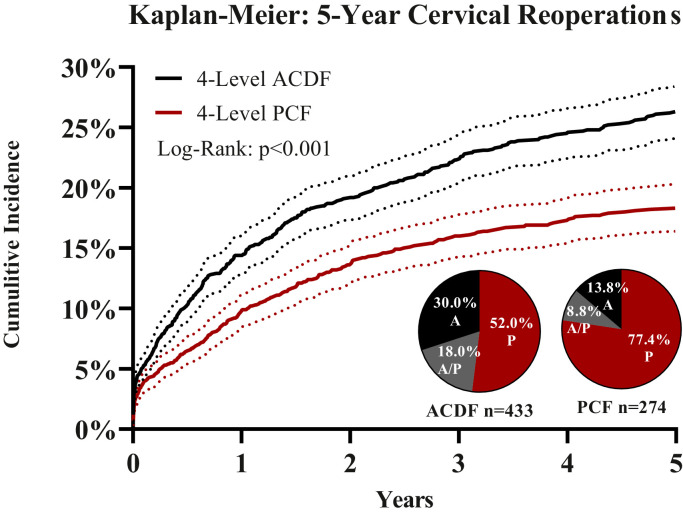
Results: A total of 3,714 patients 1:1 matched for four-level ACDF and PCF performed for degenerative pathologies were identified (1,857 for each of the study groups). On multivariate analysis controlling for age, sex, and comorbidities, PCF was found to have significantly greater odds ratios (OR) for any (OR 2.12), serious (OR 2.31), and minor (OR 1.95) adverse events, as well as for length of stay ≥3 days (OR 1.76), p<0.001 for each. However, PCF had nearly three times lower odds of dysphagia compared to ACDF (OR 0.36, p<0.001). At five years, four-level ACDF cases were found to have significantly higher reoperation rates compared to four-level PCF cases (26.3% vs 18.3%, p<0.001).
Conclusion: In evaluating four-level cervical cases, compared to anterior approach cases, posterior approach procedures were associated with approximately double the odds of any, serious, and minor adverse events, but around one third the rate of dysphagia and two thirds the rate of five-year reoperations. While the pathology may dictate surgical approach, this data suggests that the choice between four-level anterior versus posterior approach becomes a balance of risks/benefit considerations.
Keywords: ACDF, anterior cervical discectomy and fusion; Big data; CI, confidence interval; CPT, Current Procedural Terminology; Cervical myelopathy; Dysphagia; ECI, Elixhauser Comorbidity Index; ICD, International Classification of Disease; LOS, length of stay; Multi-level cervical fusion; OR, odds ratio; PCF, posterior cervical fusion; Radiculopathy; SD, standard deviation; Spinal arthrodesis; Stenosis.
© 2022 The Author(s).
Conflict of interest statement
One or more authors declare potential competing financial interests or personal relationships as specified on required ICMJE Disclosure Forms.
Figures

Similar articles
-
Single-level Anterior Cervical Discectomy and Fusion Results in Lower Five-year Revisions than Posterior Cervical Foraminotomy in a Large National Cohort.Spine (Phila Pa 1976). 2023 Sep 15;48(18):1266-1271. doi: 10.1097/BRS.0000000000004754. Epub 2023 Jun 19. Spine (Phila Pa 1976). 2023. PMID: 37339256
-
Clinical outcomes following one-, two-, three-, and four-level anterior cervical discectomy and fusion: a national database study.Spine J. 2022 Apr;22(4):542-548. doi: 10.1016/j.spinee.2021.11.002. Epub 2021 Nov 10. Spine J. 2022. PMID: 34774751
-
Comparison of Surgical Outcomes Between Anterior and Posterior Cervical Fusions Stratified by Levels Decompressed.Clin Spine Surg. 2023 Jun 1;36(5):E206-E211. doi: 10.1097/BSD.0000000000001423. Epub 2023 Jan 11. Clin Spine Surg. 2023. PMID: 36728282
-
Minimally Invasive Posterior Cervical Foraminotomy as an Alternative to Anterior Cervical Discectomy and Fusion for Unilateral Cervical Radiculopathy: A Systematic Review and Meta-analysis.Spine (Phila Pa 1976). 2019 Dec 15;44(24):1731-1739. doi: 10.1097/BRS.0000000000003156. Spine (Phila Pa 1976). 2019. PMID: 31343619
-
Anterior cervical discectomy and fusion versus posterior cervical foraminotomy for the treatment of single-level unilateral cervical radiculopathy: a meta-analysis.J Orthop Surg Res. 2020 Jun 1;15(1):202. doi: 10.1186/s13018-020-01723-5. J Orthop Surg Res. 2020. PMID: 32487109 Free PMC article.
Cited by
-
Perioperative and safety outcomes following tissue-sparing posterior cervical fusion to revise a pseudarthrosis: A multicenter retrospective review of 150 cases.J Craniovertebr Junction Spine. 2024 Apr-Jun;15(2):216-223. doi: 10.4103/jcvjs.jcvjs_13_24. Epub 2024 May 24. J Craniovertebr Junction Spine. 2024. PMID: 38957762 Free PMC article.
-
Following carpel tunnel release, what factors affect whether patients return to the same or different hand surgeon for a subsequent procedure?PLoS One. 2024 Oct 22;19(10):e0312159. doi: 10.1371/journal.pone.0312159. eCollection 2024. PLoS One. 2024. PMID: 39436931 Free PMC article.
-
Comparison of anterior and posterior approaches for functional improvement in cervical myelopathy: A systematic review and meta-analysis of 33,025 patients.N Am Spine Soc J. 2024 Nov 13;22:100567. doi: 10.1016/j.xnsj.2024.100567. eCollection 2025 Jun. N Am Spine Soc J. 2024. PMID: 40291785 Free PMC article. Review.
-
Do multiple reconstructive surgeries increase loss of cervical lordosis in patients with multilevel degenerative cervical diseases? A retrospective cohort study.Am J Neurodegener Dis. 2025 Apr 15;14(2):58-66. doi: 10.62347/MKUX5540. eCollection 2025. Am J Neurodegener Dis. 2025. PMID: 40401134 Free PMC article.
-
Patients with fibromyalgia have increased risk of 90-day postoperative adverse events following arthroscopic rotator cuff repair.JSES Int. 2024 Oct 9;9(2):360-365. doi: 10.1016/j.jseint.2024.09.018. eCollection 2025 Mar. JSES Int. 2024. PMID: 40182261 Free PMC article.
References
-
- Xiao SW, Jiang H, Yang LJ, Xiao ZM. Anterior cervical discectomy versus corpectomy for multilevel cervical spondylotic myelopathy: a meta-analysis. Eur Spine J. 2015;24(1):31–39. - PubMed
-
- Neifert SN, Martini ML, Yuk F, et al. Predicting trends in cervical spinal surgery in the United States from 2020 to 2040. World Neurosurg. 2020;141:e175–ee81. - PubMed
-
- Hirabayashi K, Bohlman HH. Multilevel cervical spondylosis. Laminoplasty versus anterior decompression. Spine (Phila Pa 1976) 1995;20(15):1732–1734. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
