

Impact of Early Oral Feeding on Nasogastric Tube Reinsertion After Elective Colorectal Surgery: A Systematic Review and Meta-Analysis
- PMID: 35392054
- PMCID: PMC8980315
- DOI: 10.3389/fsurg.2022.807811
Impact of Early Oral Feeding on Nasogastric Tube Reinsertion After Elective Colorectal Surgery: A Systematic Review and Meta-Analysis
Abstract
Background: Colorectal cancer is a common malignant tumor appearing in the gastrointestinal tract. Surgical resection is recognized as the best means to improve patient survival. However, it is controversial whether early oral feeding (EOF) after elective colorectal resection demonstrates safety and efficacy in concerned clinical outcomes.
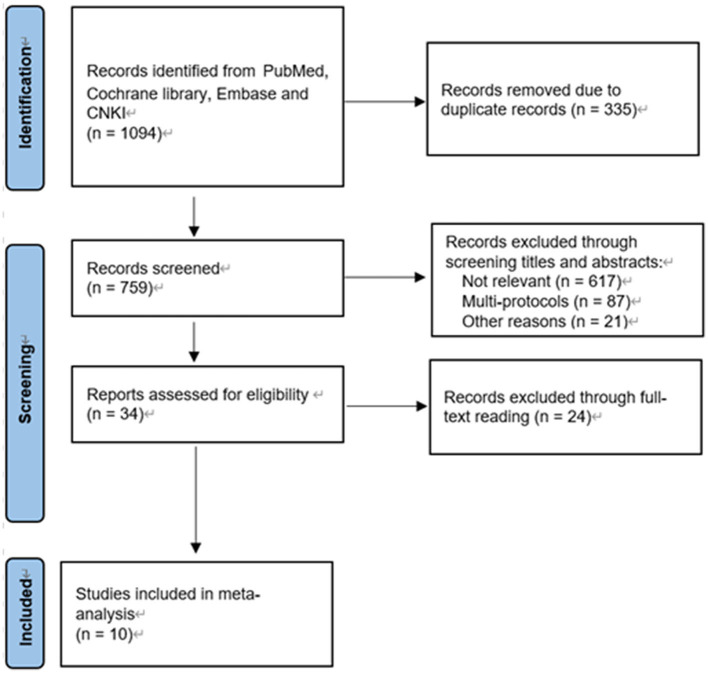
Methods: We searched PubMed, Embase, Cochrane Library, and CNKI from inception to September 2021. Two authors independently screened the retrieved records and extracted data. EOF was defined as feeding within 24 h after surgery, while traditional oral feeding (TOF) was defined as feeding that started after the gastrointestinal flatus or ileus was resolved. The primary outcome was nasogastric tube insertion, and the secondary outcomes were the length of hospital stay and total complications. Categorical data were combined using odds ratio (OR), and continuous data were combined using mean difference (MD).
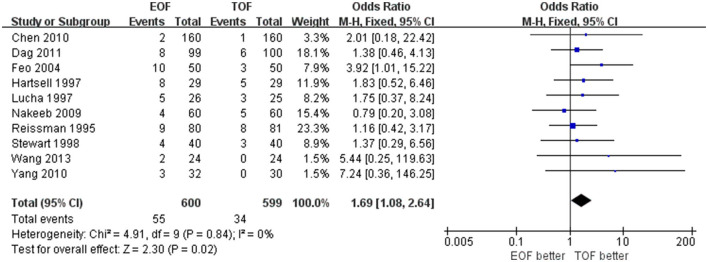
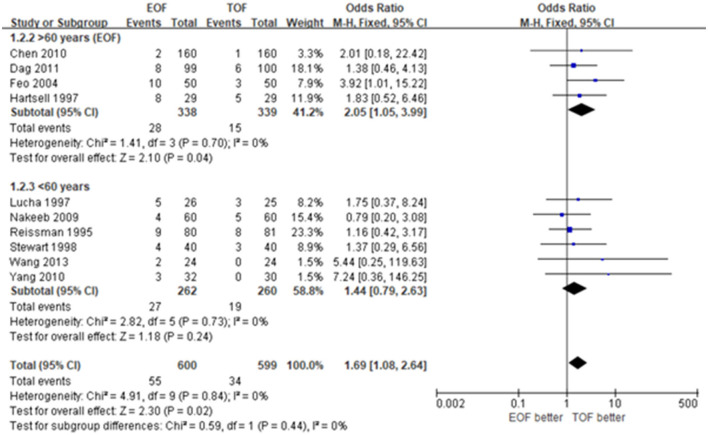
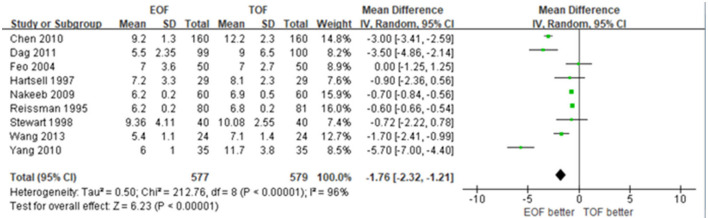
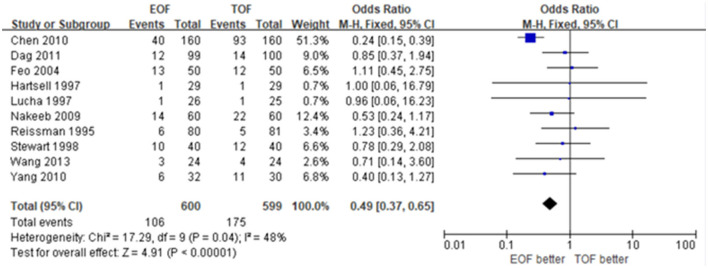
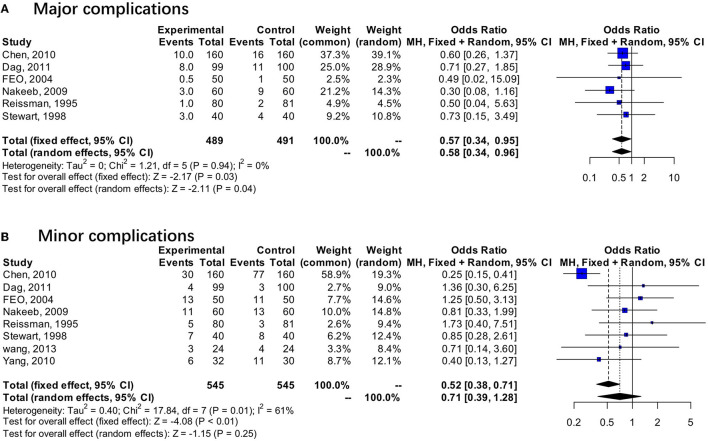
Results: We screened 10 studies from 34 records after full-text reading, with 1,199 patients included in the analysis. Nasogastric tube reinsertion (OR 1.69; 95% CI 1.08 to 2.64, p=0.02) was more frequent in the EOF group, and older ages (>60 years) were associated with higher risk of nasogastric tube reinsertion (OR 2.05; 95% CI 1.05 to 3.99, p = 0.04). Reduced length of hospital stay (MD -1.76; 95% CI -2.32 to -1.21; p < 0.01) and the rate of total complications (OR 0.49; 95% CI 0.37 to 0.65, p < 0.01) were observed in EOF compared with TOF.
Conclusions: EOF was safe and effective for patients undergoing elective colorectal surgery, but the higher rate of nasogastric tube reinsertion compared with TOF should not be ignored.
Keywords: early oral feeding; elective colorectal surgery; meta-analysis; nasogastric tube reinsertion; systematic review.
Copyright © 2022 Wang, Zhang, Hu, Wu, Liang, Jin, Wu, Cen, Wei and Wang.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
[Early versus traditional postoperative oral feeding in patients undergoing elective colorectal surgery: a meta-analysis of safety and efficacy].Zhonghua Wei Chang Wai Ke Za Zhi. 2017 Sep 25;20(9):1060-1066. Zhonghua Wei Chang Wai Ke Za Zhi. 2017. PMID: 28901001 Chinese.
-
Impact of Early Oral Feeding on Postoperative Outcomes after Elective Colorectal Surgery: A Systematic Review and Meta-Analysis.Dig Surg. 2025;42(1):26-35. doi: 10.1159/000542595. Epub 2024 Nov 18. Dig Surg. 2025. PMID: 39557028
-
Early versus traditional postoperative oral feeding in patients undergoing elective colorectal surgery: a meta-analysis of randomized clinical trials.Dig Surg. 2013;30(3):225-32. doi: 10.1159/000353136. Epub 2013 Jul 6. Dig Surg. 2013. PMID: 23838894
-
Is early oral feeding safe after elective colorectal surgery? A prospective randomized trial.Ann Surg. 1995 Jul;222(1):73-7. doi: 10.1097/00000658-199507000-00012. Ann Surg. 1995. PMID: 7618972 Free PMC article. Review.
-
Early oral feeding after elective colorectal surgery: is it safe.Trop Gastroenterol. 1995 Oct-Dec;16(4):72-3. Trop Gastroenterol. 1995. PMID: 8854962 Clinical Trial.
Cited by
-
EARLY REFEEDING AFTER COLORECTAL CANCER SURGERY REDUCES COMPLICATIONS AND LENGTH OF HOSPITAL STAY.Arq Bras Cir Dig. 2025 Jan 20;37:e1854. doi: 10.1590/0102-6720202400060e1854. eCollection 2025. Arq Bras Cir Dig. 2025. PMID: 39841760 Free PMC article.
-
Nutritional care in patients undergoing laparoscopic/minimally invasive surgeries for gastrointestinal tumours.Wideochir Inne Tech Maloinwazyjne. 2023 Dec;18(4):625-638. doi: 10.5114/wiitm.2023.130468. Epub 2023 Aug 11. Wideochir Inne Tech Maloinwazyjne. 2023. PMID: 38239578 Free PMC article. Review.
-
Time to return of bowel function following perioperative probiotics in colorectal cancer surgery (PICCS-1): study protocol for a randomized controlled trial.Trials. 2025 Feb 19;26(1):60. doi: 10.1186/s13063-025-08773-2. Trials. 2025. PMID: 39972354 Free PMC article.
References
Publication types
LinkOut - more resources
Full Text Sources