

Sex Matters: A Comprehensive Comparison of Female and Male Hearts
- PMID: 35392369
- PMCID: PMC8980481
- DOI: 10.3389/fphys.2022.831179
Sex Matters: A Comprehensive Comparison of Female and Male Hearts
Abstract
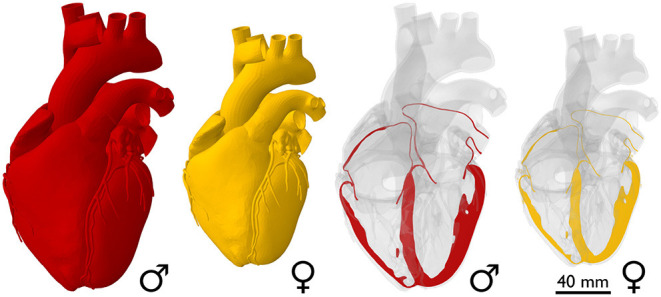
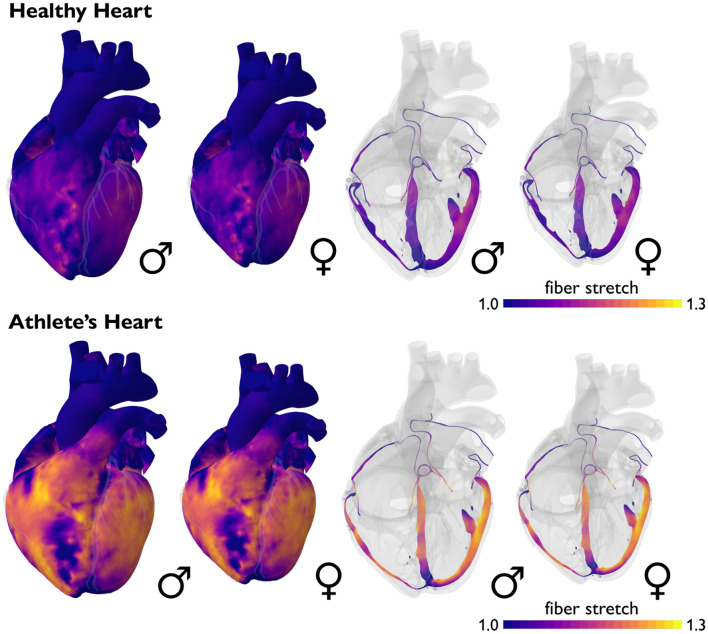
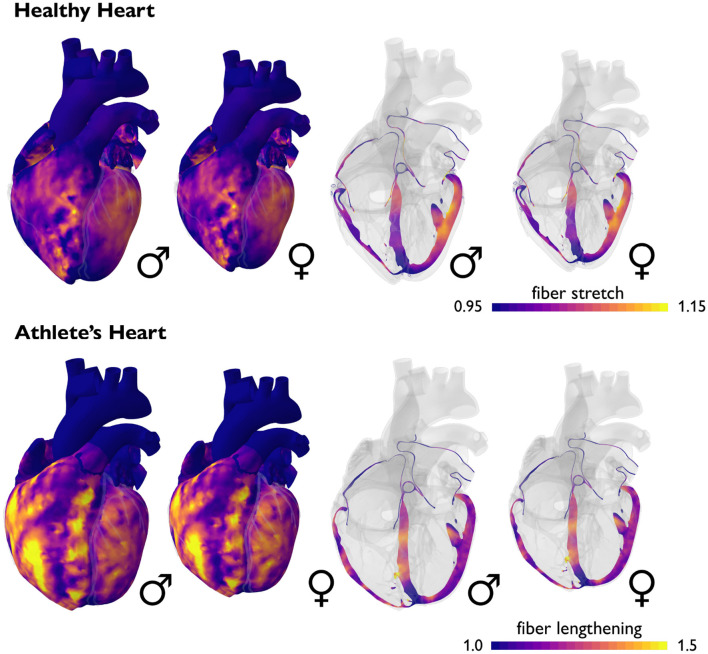
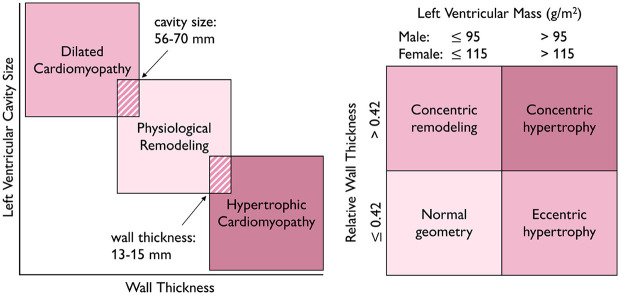
Cardiovascular disease in women remains under-diagnosed and under-treated. Recent studies suggest that this is caused, at least in part, by the lack of sex-specific diagnostic criteria. While it is widely recognized that the female heart is smaller than the male heart, it has long been ignored that it also has a different microstructural architecture. This has severe implications on a multitude of cardiac parameters. Here, we systematically review and compare geometric, functional, and structural parameters of female and male hearts, both in the healthy population and in athletes. Our study finds that, compared to the male heart, the female heart has a larger ejection fraction and beats at a faster rate but generates a smaller cardiac output. It has a lower blood pressure but produces universally larger contractile strains. Critically, allometric scaling, e.g., by lean body mass, reduces but does not completely eliminate the sex differences between female and male hearts. Our results suggest that the sex differences in cardiac form and function are too complex to be ignored: the female heart is not just a small version of the male heart. When using similar diagnostic criteria for female and male hearts, cardiac disease in women is frequently overlooked by routine exams, and it is diagnosed later and with more severe symptoms than in men. Clearly, there is an urgent need to better understand the female heart and design sex-specific diagnostic criteria that will allow us to diagnose cardiac disease in women equally as early, robustly, and reliably as in men.
Systematic review registration: https://livingmatter.stanford.edu/.
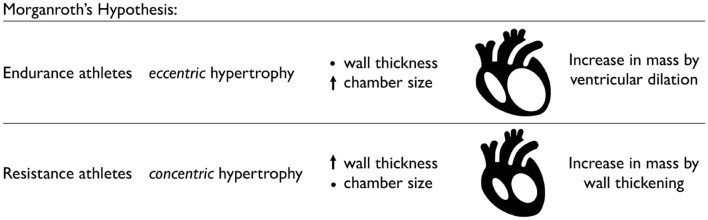
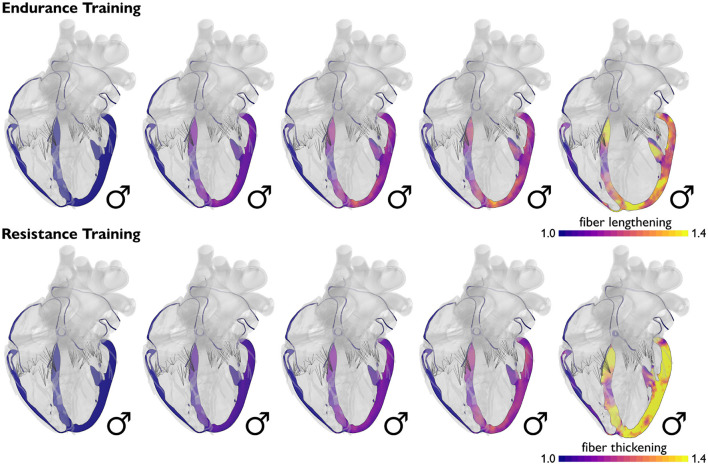
Keywords: athlete's heart; cardiac remodeling; concentric hypertrophy; dilated cardiomyopathy; eccentric hypertrophy; hypertrophic cardiomyopathy; sex differences; sex-specific diagnostics.
Copyright © 2022 St. Pierre, Peirlinck and Kuhl.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures

References
-
- Altman P. L., Dittmer D. S. (1962). Growth Including Reproduction and Morphological Development. Washington, DC: Federation of American Societies for Experimental Biology.
Publication types
LinkOut - more resources
Full Text Sources