

Increased Risk of Herpes Zoster in Adults ≥50 Years Old Diagnosed With COVID-19 in the United States
- PMID: 35392454
- PMCID: PMC8982770
- DOI: 10.1093/ofid/ofac118
Increased Risk of Herpes Zoster in Adults ≥50 Years Old Diagnosed With COVID-19 in the United States
Abstract
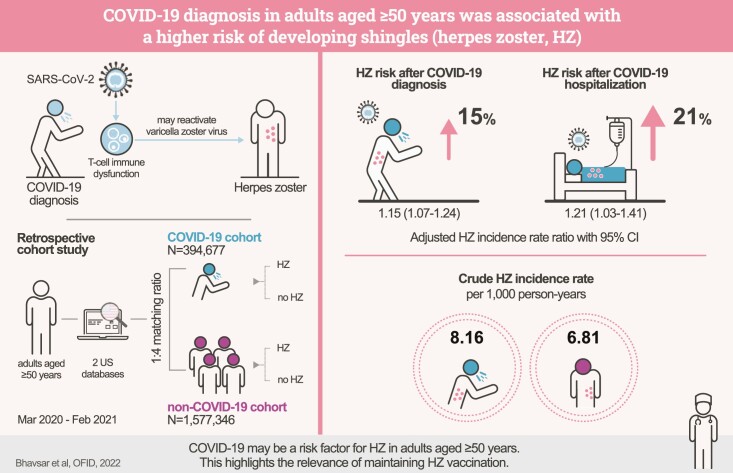
Background: Case reports have described herpes zoster (HZ) in patients with coronavirus disease 2019 (COVID-19). However, this constitutes low-quality evidence for an association. We therefore performed a retrospective cohort study to assess the risk of developing HZ following a COVID-19 diagnosis.
Methods: We compared the HZ incidence in ≥50-year-olds diagnosed with COVID-19 vs those never diagnosed with COVID-19. We used data from the US MarketScan Commercial Claims and Encounters and Medicare Supplemental (3/2020-2/2021) and Optum Clinformatics Data Mart (3-12/2020) databases. Individuals with COVID-19 were exact-matched 1:4 to those without COVID-19 by age, sex, presence of HZ risk factors, and health care cost level. Adjusted incidence rate ratios (aIRRs) were estimated by Poisson regression.
Results: A total of 394 677 individuals ≥50 years old with COVID-19 were matched with 1 577 346 individuals without COVID-19. Mean follow-up time after COVID-19 diagnosis and baseline characteristics were balanced between cohorts. Individuals diagnosed with COVID-19 had a 15% higher HZ risk than those without COVID-19 (aIRR, 1.15; 95% CI, 1.07-1.24; P < .001). The increased HZ risk was more pronounced (21%) following COVID-19 hospitalization (aIRR, 1.21; 95% CI, 1.03-1.41; P = .02).
Conclusions: We found that COVID-19 diagnosis in ≥50-year-olds was associated with a significantly increased risk of developing HZ, highlighting the relevance of maintaining HZ vaccination.
Keywords: COVID-19; SARS-CoV-2; coronavirus; herpes zoster; shingles.
© The Author(s) 2022. Published by Oxford University Press on behalf of Infectious Diseases Society of America.
Figures


References
LinkOut - more resources
Full Text Sources
Miscellaneous
