

Value of estimated pulse wave velocity to identify left ventricular hypertrophy prevalence: insights from a general population
- PMID: 35392823
- PMCID: PMC8990685
- DOI: 10.1186/s12872-022-02541-9
Value of estimated pulse wave velocity to identify left ventricular hypertrophy prevalence: insights from a general population
Abstract
Background: Aortic stiffness shares a similar profile of risk factors with left ventricular hypertrophy (LVH) and can also lead to LVH by itself. Published data have demonstrated the correlation between aortic stiffness and LVH. Recent data have revealed estimated pulse wave velocity (ePWV) to be a simple and cost-effective marker of the severity of aortic stiffness. Our analysis aimed to explore the association between ePWV and LVH prevalence, and to investigate the incremental value of ePWV for the identification of LVH prevalence.
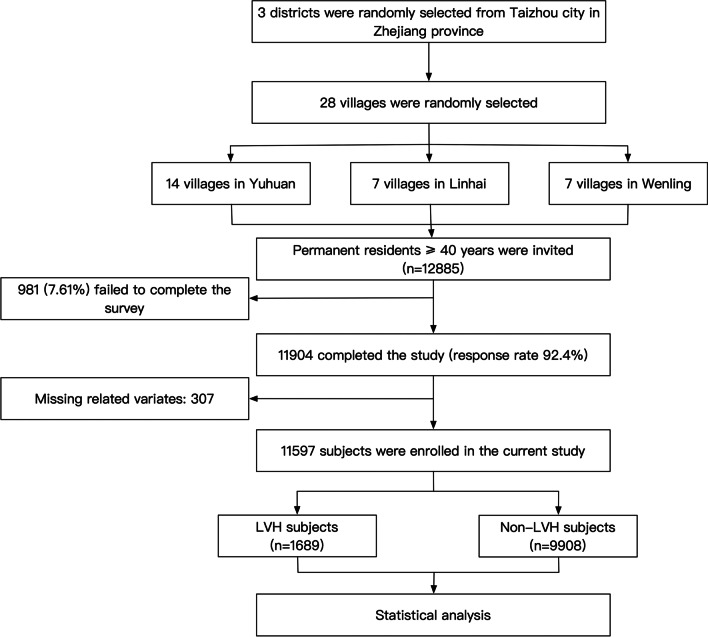
Methods: The present analysis based on a cross-sectional survey which included 11,597 participants from rural areas of southeastern China between Sep 2020 and Feb 2021. ePWV was formulated based on mean blood pressure and age according to a published algorithm.
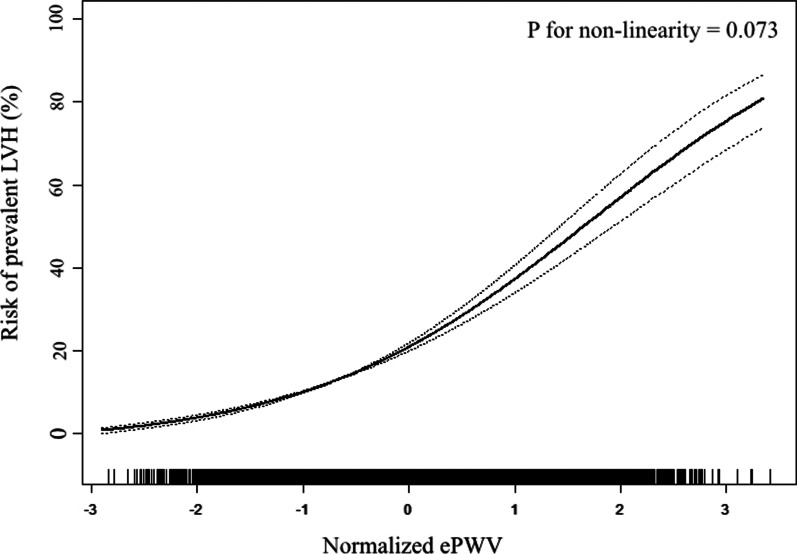
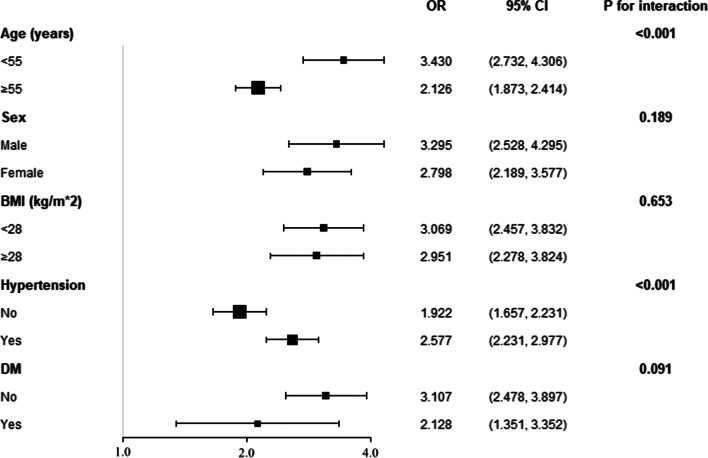
Results: The prevalence of LVH was 14.56%. With the adjustment of age, sex, education, income and physical activity level, current drinking and smoking status, BMI, waist circumference, serum creatinine, total cholesterol, high density cholesterol, mean blood pressure, fasting plasma glucose, anti-hypertensive therapy, anti-diabetic therapy, lipid-lowering therapy, and cardiovascular disease history, every standard deviation increment of ePWV associated with a 2.993 times risk of LVH prevalence. When dividing ePWV into quartiles, the top quartile had a 4.520 times risk of LVH prevalence when compared with the bottom quartile. Furthermore, smooth spline analysis displayed that the association was linear in the whole range of ePWV (p for non-linearity = 0.073). Additionally, subgroup analysis revealed the association was robust to sex, obesity and diabetes, and younger people and hypertensive population were more vulnerable to the increase of ePWV than their corresponding counterparts. Finally, ROC analysis showed a significant advancement when introducing ePWV into established risk factors (0.787 vs. 0.810, p for comparison < 0.001), and reclassification analysis also confirmed significant improvement from ePWV to identify LVH prevalence (category-free net reclassification analysis = 0.421, p < 0.001; integrated discrimination index = 0.023, p < 0.001).
Conclusion: Our analysis demonstrated a linear association between ePWV and LVH prevalence. Furthermore, our results suggest younger people and hypertensive population are more likely to have LVH prevalence with the increase of ePWV. More importantly, our findings implicate the incremental value of ePWV to optimize the identification of LVH prevalence in a general Chinese population.
Keywords: Aortic stiffness; Estimated pulse wave velocity; Left ventricular hypertrophy.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Usefulness of estimated pulse wave velocity for identifying prevalent coronary heart disease: findings from a general Chinese population.BMC Cardiovasc Disord. 2022 Jan 12;22(1):9. doi: 10.1186/s12872-022-02456-5. BMC Cardiovasc Disord. 2022. PMID: 35016632 Free PMC article.
-
Value of estimated glucose disposal rate to detect prevalent left ventricular hypertrophy: implications from a general population.Postgrad Med. 2023 Jan;135(1):58-66. doi: 10.1080/00325481.2022.2131153. Epub 2022 Oct 5. Postgrad Med. 2023. PMID: 36174224
-
Association of Estimated Pulse Wave Velocity With Survival: A Secondary Analysis of SPRINT.JAMA Netw Open. 2019 Oct 2;2(10):e1912831. doi: 10.1001/jamanetworkopen.2019.12831. JAMA Netw Open. 2019. PMID: 31596491 Free PMC article.
-
Prevalence of left ventricular hypertrophy in children and young people with primary hypertension: Meta-analysis and meta-regression.Front Cardiovasc Med. 2022 Oct 31;9:993513. doi: 10.3389/fcvm.2022.993513. eCollection 2022. Front Cardiovasc Med. 2022. PMID: 36386367 Free PMC article.
-
Prevalence rate of left ventricular hypertrophy and the burden of arrhythmias among hypertensive patients attending Jinja regional referral hospital, eastern Uganda.Curr Probl Cardiol. 2024 Jul;49(7):102576. doi: 10.1016/j.cpcardiol.2024.102576. Epub 2024 Apr 21. Curr Probl Cardiol. 2024. PMID: 38653445 Review.
Cited by
-
Association of estimated pulse wave velocity with all-cause mortality and cardiovascular mortality in obstructive sleep apnea patients: results from NHANES.Front Cardiovasc Med. 2025 Jun 12;12:1571610. doi: 10.3389/fcvm.2025.1571610. eCollection 2025. Front Cardiovasc Med. 2025. PMID: 40574813 Free PMC article.
-
System inflammation response index: a novel inflammatory indicator to predict all-cause and cardiovascular disease mortality in the obese population.Diabetol Metab Syndr. 2023 Oct 11;15(1):195. doi: 10.1186/s13098-023-01178-8. Diabetol Metab Syndr. 2023. PMID: 37821960 Free PMC article.
-
Elevated pulse wave velocity as a marker of arterial stiffness and its association with mortality in US adults.Sci Rep. 2025 Jul 2;15(1):23026. doi: 10.1038/s41598-025-07198-w. Sci Rep. 2025. PMID: 40596198 Free PMC article.
-
Prevalence of clinical signs, symptoms and comorbidities at diagnosis of acromegaly: a systematic review in accordance with PRISMA guidelines.Pituitary. 2023 Aug;26(4):319-332. doi: 10.1007/s11102-023-01322-7. Epub 2023 May 20. Pituitary. 2023. PMID: 37210433 Free PMC article.
-
Association of estimated pulse wave velocity with cognitive function in a multiethnic diverse population: The Northern Manhattan Study.Alzheimers Dement. 2024 Jul;20(7):4903-4913. doi: 10.1002/alz.14064. Epub 2024 Jun 19. Alzheimers Dement. 2024. PMID: 38895994 Free PMC article.
References
-
- Drazner MH, Rame JE, Marino EK, Gottdiener JS, Kitzman DW, Gardin JM, Manolio TA, Dries DL, Siscovick DS. Increased left ventricular mass is a risk factor for the development of a depressed left ventricular ejection fraction within five years: the Cardiovascular Health Study. J Am Coll Cardiol. 2004;43(12):2207–2215. doi: 10.1016/j.jacc.2003.11.064. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
