

Acute kidney injury contributes to worse physical and quality of life outcomes in survivors of critical illness
- PMID: 35392844
- PMCID: PMC8991933
- DOI: 10.1186/s12882-022-02749-z
Acute kidney injury contributes to worse physical and quality of life outcomes in survivors of critical illness
Abstract
Objectives: Survivors of critical illness and acute kidney injury (AKI) are at risk of increased morbidity. The purpose of this study was to compare physical, emotional, and cognitive health in survivors of critical illness with and without AKI.
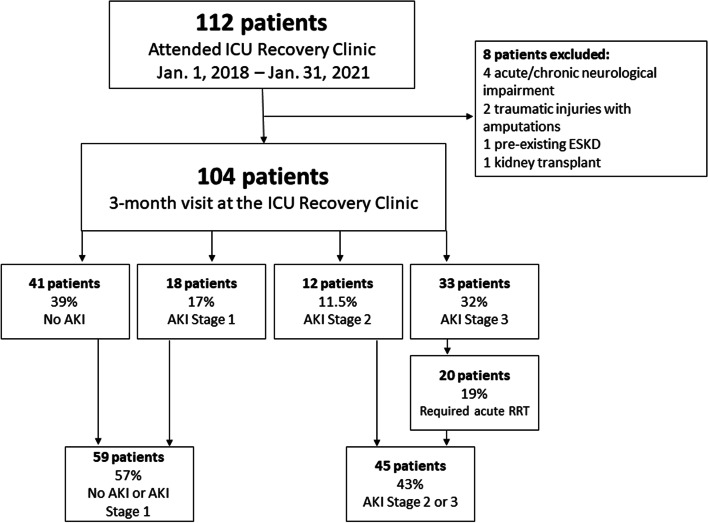
Methods: Retrospective cohort study of adult (≥ 18 years old) survivors of critical illness due to sepsis and/or acute respiratory failure who attended follow-up in a specialized ICU Recovery Clinic. Outcomes were evaluated during 3-month visit and comprised validated tests for evaluation of physical function, muscle strength, cognitive and emotional health, and self-reported health-related quality of life (HRQOL). Descriptive statistics and group comparisons were performed.
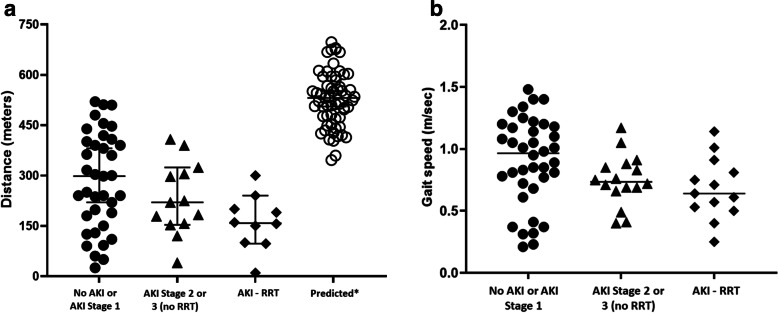
Results: A total of 104 patients with median age of 55 [49-64] years, 54% male, and median SOFA score of 10 [8-12] were analyzed. Incidence of AKI during ICU admission was 61 and 19.2% of patients required renal replacement therapy (RRT). Patients with AKI stage 2 or 3 (vs. those with AKI stage 1 or no AKI) walked less on the 6-min walk test (223 ± 132 vs. 295 ± 153 m, p = 0.059) and achieved lower of the predicted walk distance (38% vs. 58%, p = 0.041). Similar patterns of worse physical function and more significant muscle weakness were observed in multiple tests, with overall worse metrics in patients that required RRT. Patients with AKI stage 2 or 3 also reported lower HRQOL scores when compared to their counterparts, including less ability to return to work or hobby, or reengage in driving. There were no significant differences in cognitive function or emotional health between groups.
Conclusions: Survivors of critical illness and AKI stage 2 or 3 have increased physical debility and overall lower quality of life, with more impairment in return to work, hobby, and driving when compared to their counterparts without AKI or AKI stage 1 at 3 months post-discharge.
Keywords: Acute kidney injury; critical illness; Patient-centered outcomes; Quality of life; Survivors.
© 2022. The Author(s).
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
