

Diagnosis of tuberculosis in dialysis and kidney transplant patients
- PMID: 35393765
- PMCID: PMC9546140
- DOI: 10.1111/hdi.13010
Diagnosis of tuberculosis in dialysis and kidney transplant patients
Abstract
Background and objectives: In patients with chronic kidney disease the risk of developing Tuberculosis is increased, while the presentation is often atypical making the diagnosis more difficult. The aim of this study is to describe the presentation of Tuberculosis in dialysis and kidney transplant patients, including the range of diagnostic approaches and the utility of different sample types.
Design, setting, participants, and measurements: In this retrospective study, case records of dialysis and kidney transplant patients were reviewed, including all those treated for Tuberculosis between January 2009 and December 2020.
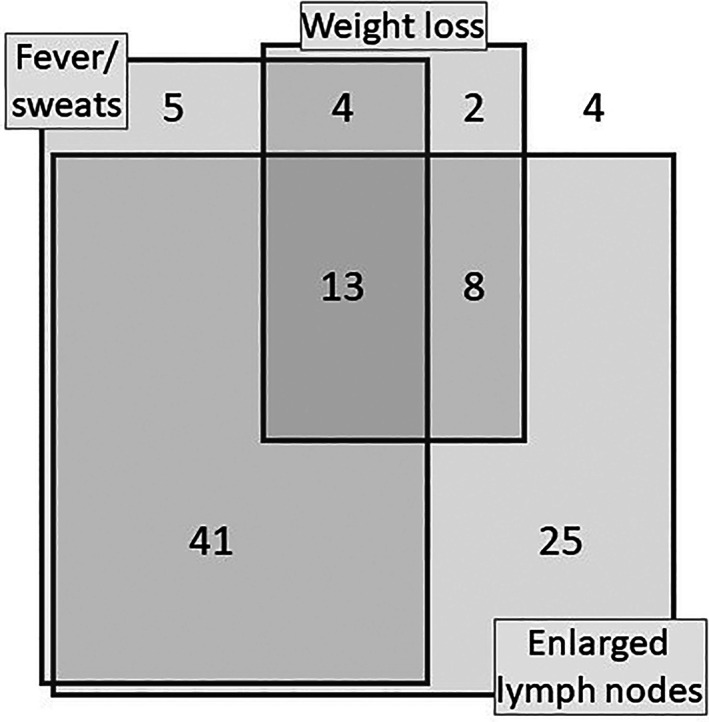
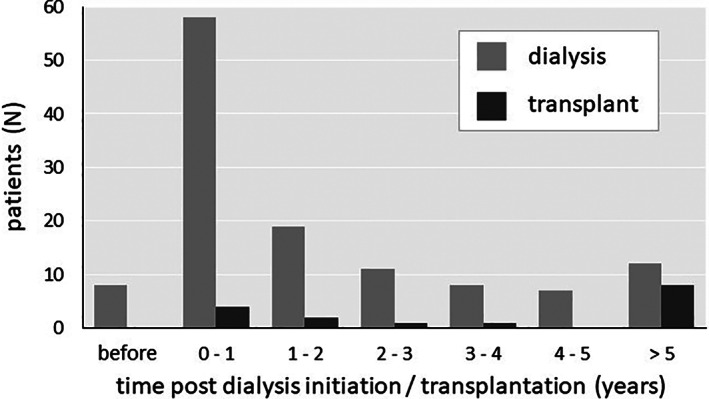
Results: Over 12 years, there were 143 cases of Tuberculosis in 141 patients (aged 17-86, 50.4% male). Tuberculosis was most common in Asian patients (64%) and those receiving hemodialysis (82%), particularly during the first year after dialysis initiation (54% of dialysis cases). Non-pleural/pulmonary disease accounted 40% of cases, and non-organ-specific presenting features were prominent including fever, lymphadenopathy, and weight loss. The diagnosis was confirmed microbiologically or histologically in 87 cases (61%), with low sensitivity observed for many types of samples including sputum (18%) and pleural fluid (12%). Higher sensitivity was observed with tissue samples including bronchoscopic lymph node aspiration (75%) and other lymph node sampling (92%). In the 52 cases where drug sensitivities were available, resistance to a first line treatment, most commonly isoniazid, was seen in 12 cases (23%). Furthermore, 1- and 5-year survival from diagnosis were 78% and 61%, respectively. Baseline variables independently associated with poorer survival were age (OR 1.8 per decade, 95% CI 1.4-2.3), weight loss over 10% (OR 1.9, 95% CI 1.0-3.5), and a non-confirmed diagnosis (OR 1.6, 95% CI 1.2-2.1).
Conclusions: Tuberculosis is common in dialysis and kidney transplant patients, particularly during the first year of dialysis. Short-term mortality is high, but the diagnostic sensitivity of many types of samples is low, so that diagnosis is difficult, with treatment often initiated without confirmation. These data highlight the importance of judgment and clinical experience with this complex patient group.
Keywords: chronic kidney disease; dialysis; infections; kidney transplant; tuberculosis.
© 2022 The Authors. Hemodialysis International published by Wiley Periodicals LLC on behalf of International Society for Hemodialysis.
Conflict of interest statement
Authors have no potential conflict to declare.
Figures




References
-
- Holty J, Sista R. Mycobacterium tuberculosis infection in transplant recipients: early diagnosis and treatment of resistant tuberculosis. Curr Opin Organ Transplant. 2009;14(6):613–8. - PubMed
-
- Romanowski K, Clark E, Levin A, Cook V, Johnston J. Tuberculosis and chronic kidney disease: an emerging global syndemic. Kidney Int. 2016;90(1):34–40. - PubMed
-
- Ostermann M, Palchaudhuri P, Riding A, Begum P, Milburn H. Incidence of tuberculosis is high in chronic kidney disease patients in south East England and drug resistance common. Ren Fail. 2016;38(2):256–61. - PubMed
-
- Vikrant S. Clinical profile of tuberculosis in patients with chronic kidney disease: a report from an endemic country. Saudi J Kidney Dis Transpl. 2019;30(2):470–7. - PubMed
-
- UK Government , 2021. Tuberculosis in England: annual report. Available at https://www.gov.uk/government/publications/tuberculosis‐in‐england‐annua.... Accessed 13 June 2021.
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
