

Distinct Immune Gene Programs Associated with Host Tumor Immunity, Neoadjuvant Chemotherapy, and Chemoimmunotherapy in Resectable NSCLC
- PMID: 35394499
- PMCID: PMC9167789
- DOI: 10.1158/1078-0432.CCR-21-3207
Distinct Immune Gene Programs Associated with Host Tumor Immunity, Neoadjuvant Chemotherapy, and Chemoimmunotherapy in Resectable NSCLC
Abstract
Purpose: Our understanding of the immunopathology of resectable non-small cell lung cancer (NSCLC) is still limited. Here, we explore immune programs that inform of tumor immunity and response to neoadjuvant chemotherapy and chemoimmunotherapy in localized NSCLC.
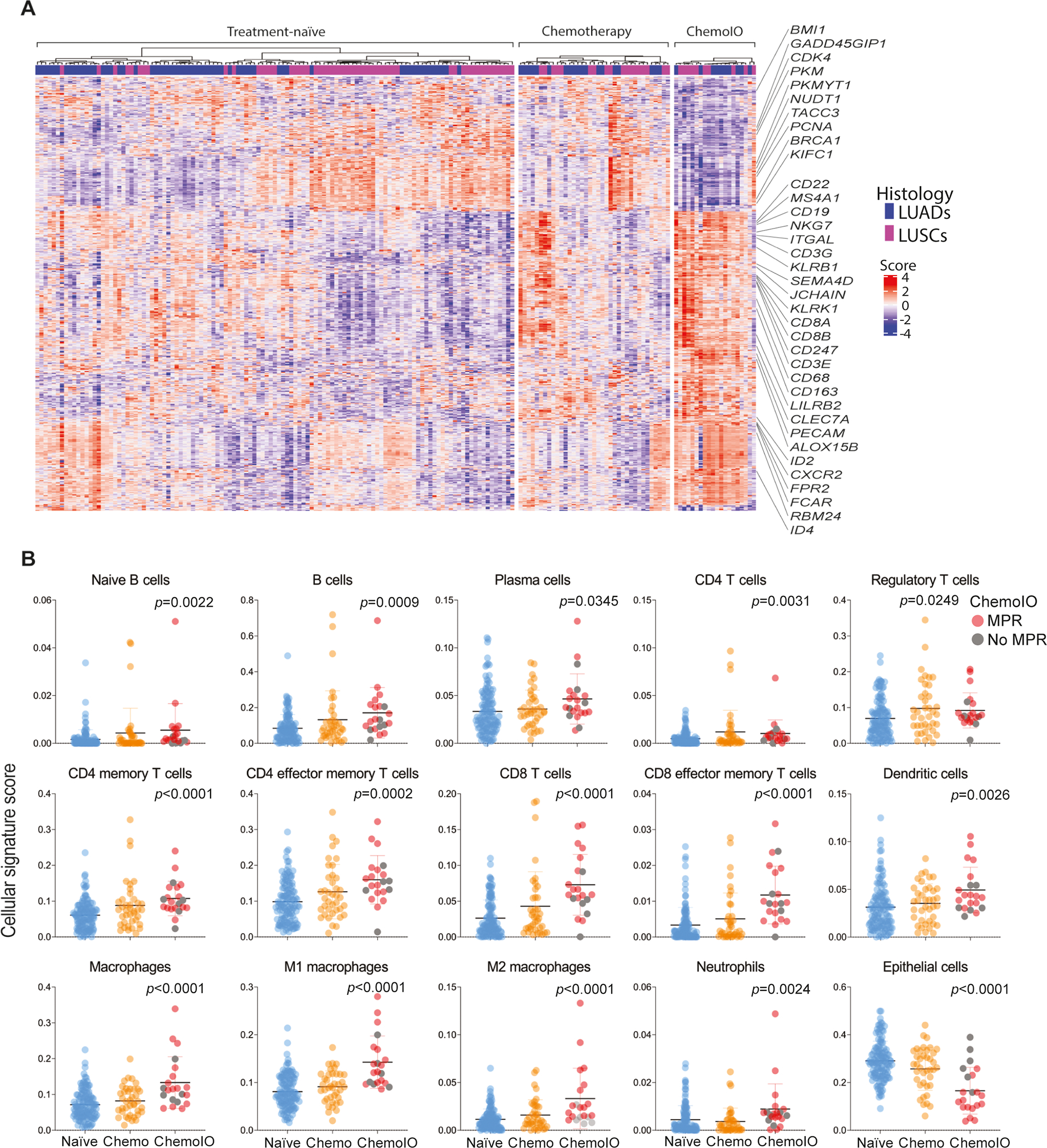
Experimental design: Targeted immune gene sequencing using the HTG Precision Immuno-Oncology panel was performed in localized NSCLCs from three cohorts based on treatment: naïve (n = 190), neoadjuvant chemotherapy (n = 38), and neoadjuvant chemoimmunotherapy (n = 21). Tumor immune microenvironment (TIME) phenotypes were based on the location of CD8+ T cells (inflamed, cold, excluded), tumoral PD-L1 expression (<1% and ≥1%), and tumor-infiltrating lymphocytes (TIL). Immune programs and signatures were statistically analyzed on the basis of tumoral PD-L1 expression, immune phenotypes, and pathologic response and were cross-compared across the three cohorts.
Results: PD-L1-positive tumors exhibited increased signature scores for various lymphoid and myeloid cell subsets (P < 0.05). TIME phenotypes exhibited disparate frequencies by stage, PD-L1 expression, and mutational burden. Inflamed and PD-L1+/TILs+ NSCLCs displayed overall significantly heightened levels of immune signatures, with the excluded group representing an intermediate state. A cytotoxic T-cell signature was associated with favorable survival in neoadjuvant chemotherapy-treated NSCLCs (P < 0.05). Pathologic response to chemoimmunotherapy was positively associated with higher expression of genes involved in immune activation, chemotaxis, as well as T and natural killer cells (P < 0.05 for all). Among the three cohorts, chemoimmunotherapy-treated NSCLCs exhibited the highest scores for various immune cell subsets including T effector and B cells (P < 0.05).
Conclusions: Our findings highlight immune gene programs that may underlie host tumor immunity and response to neoadjuvant chemotherapy and chemoimmunotherapy in resectable NSCLC.
©2022 American Association for Cancer Research.
Figures




References
-
- Siegel RL, Miller KD, Fuchs HE & Jemal A Cancer statistics, 2022. CA. Cancer J. Clin. 72, 7–33 (2022). - PubMed
-
- Siegel RL, Miller KD, Fuchs HE & Jemal A Cancer Statistics, 2021. CA. Cancer J. Clin 71, 7–33 (2021). - PubMed
-
- Felip E et al. Adjuvant atezolizumab after adjuvant chemotherapy in resected stage IB-IIIA non-small-cell lung cancer (IMpower010): a randomised, multicentre, open-label, phase 3 trial. Lancet (London, England) 398, 1344–1357 (2021). - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
