

Foeto-maternal complications associated with low birth weight: A prospective multicenter study in northern Ghana
- PMID: 35395061
- PMCID: PMC8992983
- DOI: 10.1371/journal.pone.0266796
Foeto-maternal complications associated with low birth weight: A prospective multicenter study in northern Ghana
Abstract
Objective: The study evaluated the socio-demographic characteristics, obstetric variables and foeto-maternal complications associated with low birth weight (LBW) in order to provide better treatment and management options.
Methods: The prospective study conducted from February, 2019 to June, 2020 recruited 312 primigravid pregnant women who reported for antenatal care in three tertiary referral hospitals in northern Ghana. Their socio-demographic, obstetric and adverse foeto-maternal outcome information were obtained with a well-structured questionnaire according to the World Health Organisation (WHO) guidelines. Participants' blood samples were collected for haematological tests. Odds ratio [OR, 95% confidence interval (CI)] for the association between socio-demographic, obstetric characteristics, foeto-maternal complications and haematological tests in relation to LBW were assessed using logistic regression model.
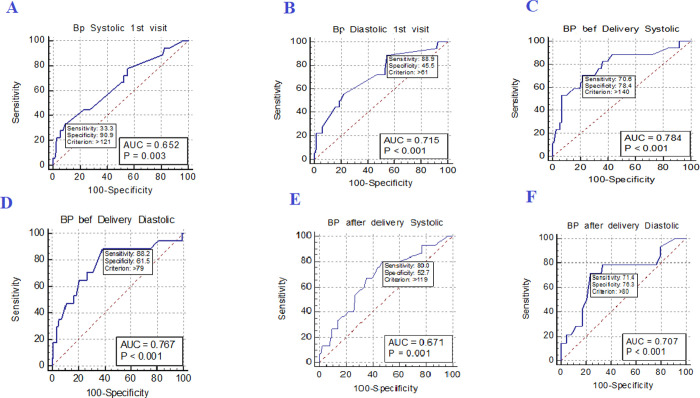
Results: This study reported a LBW prevalence of 13.5%. Increasing maternal systolic blood pressure (SBP) and diastolic blood pressure (DBP) at 1st visit, before and after delivery significantly increased the odds of LBW. Preterm delivery (PTD<37 weeks) (COR = 9.92, 95% CI (4.87-2020), p<0.001), preeclampsia (PE) (COR = 5.94, 95% CI (2.96-11.94), p<0.001), blood transfusion (COR = 14.11, 95% CI (2.50-79.65), p = 0.003), caesarian delivery (COR = 3.86, 95% CI (1.96-7.58), p<0.001) and male sex neonates (COR = 2.25, 95%CI (1.14-4.47), P = 0.020) presented with increased odds of LBW. Increasing gestational age at delivery presented with 28% reduced odds of LBW (COR = 0.72, 95% CI (1.12-4.40), P = 0.023). Upon controlling for potential confounders in multivariate logistic regression, only gestational age at delivery (AOR = 0.67, 95% CI (0.47-0.96), P = 0.030) remained significantly associated with reduced odds of LBW.
Conclusion: This study found that high blood pressure at 1st visit, before and after delivery results in increased chances of delivering a baby with LBW. Furthermore, PTD<37 weeks, having PE in current pregnancy, and male sex potentiate the risk of LBW. On the other hand, increasing gestational age reduces the risk of LBW. Thus, we recommend that midwives should intensify education to pregnant women on the benefits of regular ANC visits to aid in the early detection of adverse foeto-maternal complications. We also recommend proper clinical management of pregnancies associated with an elevated blood pressure at registration. Also, maternal intrapartum blood pressure measurement could be used to predict LBW in low resourced settings.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures


Similar articles
-
Maternal obstetric and socio-demographic determinants of low birth weight: a retrospective cross-sectional study in Ghana.Reprod Health. 2019 May 29;16(1):70. doi: 10.1186/s12978-019-0742-5. Reprod Health. 2019. PMID: 31142327 Free PMC article.
-
High prevalence of vitamin D deficiency among normotensive and hypertensive pregnant women in Ghana.BMC Pregnancy Childbirth. 2021 Apr 26;21(1):331. doi: 10.1186/s12884-021-03802-9. BMC Pregnancy Childbirth. 2021. PMID: 33902494 Free PMC article.
-
Maternal demographic and antenatal factors, low birth weight and preterm birth: findings from the mother and child in the environment (MACE) birth cohort, Durban, South Africa.BMC Pregnancy Childbirth. 2020 Oct 16;20(1):628. doi: 10.1186/s12884-020-03328-6. BMC Pregnancy Childbirth. 2020. PMID: 33076865 Free PMC article.
-
Association between maternal HIV infection and low birth weight and prematurity: a meta-analysis of cohort studies.BMC Pregnancy Childbirth. 2015 Oct 8;15:246. doi: 10.1186/s12884-015-0684-z. BMC Pregnancy Childbirth. 2015. PMID: 26450602 Free PMC article. Review.
-
Does Treating Genital Herpes during Pregnancy Improve Birth Outcomes? [Internet].Washington (DC): Patient-Centered Outcomes Research Institute (PCORI); 2021 Apr. Washington (DC): Patient-Centered Outcomes Research Institute (PCORI); 2021 Apr. PMID: 38232216 Free Books & Documents. Review.
Cited by
-
Caesarean section delivery and its associated factors in Ghana: A multilevel analysis.PLoS One. 2025 Feb 12;20(2):e0318223. doi: 10.1371/journal.pone.0318223. eCollection 2025. PLoS One. 2025. PMID: 39937831 Free PMC article.
-
Low birth weight risk prediction model: a prognostic study in the Birhan field site in Ethiopia.J Glob Health. 2025 Jul 1;15:04209. doi: 10.7189/jogh.15.04209. J Glob Health. 2025. PMID: 40590238 Free PMC article.
References
-
- WORLD HEALTH ORGANIZATION. What’s at stake Low Birth Weight Policy Brief. Who. 2014; 1–7.
-
- Chaman R, Amiri M, Khosravi A, Raei M, Ajami M-E, Sadeghian A. Bajo peso al nacer y sus factores de riesgo en el noreste de Irán. Iran J Pediatr. 2013;23: 701–4. Available: http://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=4025130&tool=p... - PMC - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
