

Cognitive underpinnings of COVID-19 vaccine hesitancy
- PMID: 35395612
- PMCID: PMC8920576
- DOI: 10.1016/j.socscimed.2022.114911
Cognitive underpinnings of COVID-19 vaccine hesitancy
Abstract
Rationale: Vaccines save lives. Despite the undisputed value of vaccination, vaccine hesitancy continues to be a major global challenge, particularly throughout the COVID-19 global pandemic. Since vaccination decisions are counter-intuitive and cognitively demanding, we propose that vaccine hesitancy is associated with executive function-a group of high-level cognitive skills including attentional control, working memory, inhibition, self-regulation, cognitive flexibility, and strategic planning.
Objective: We set out to test (i) whether vaccine hesitancy is driven by individual differences in executive function beyond established socio-demographic factors (e.g., education, political orientation, gender, ethnicity, age, religiosity) and depressed mood, and (ii) whether this relationship is exacerbated by situational stress.
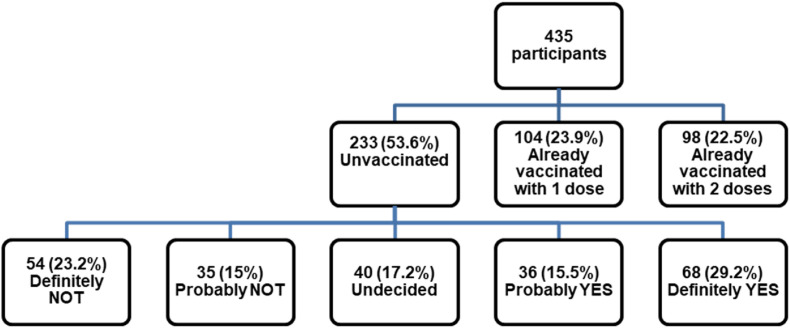
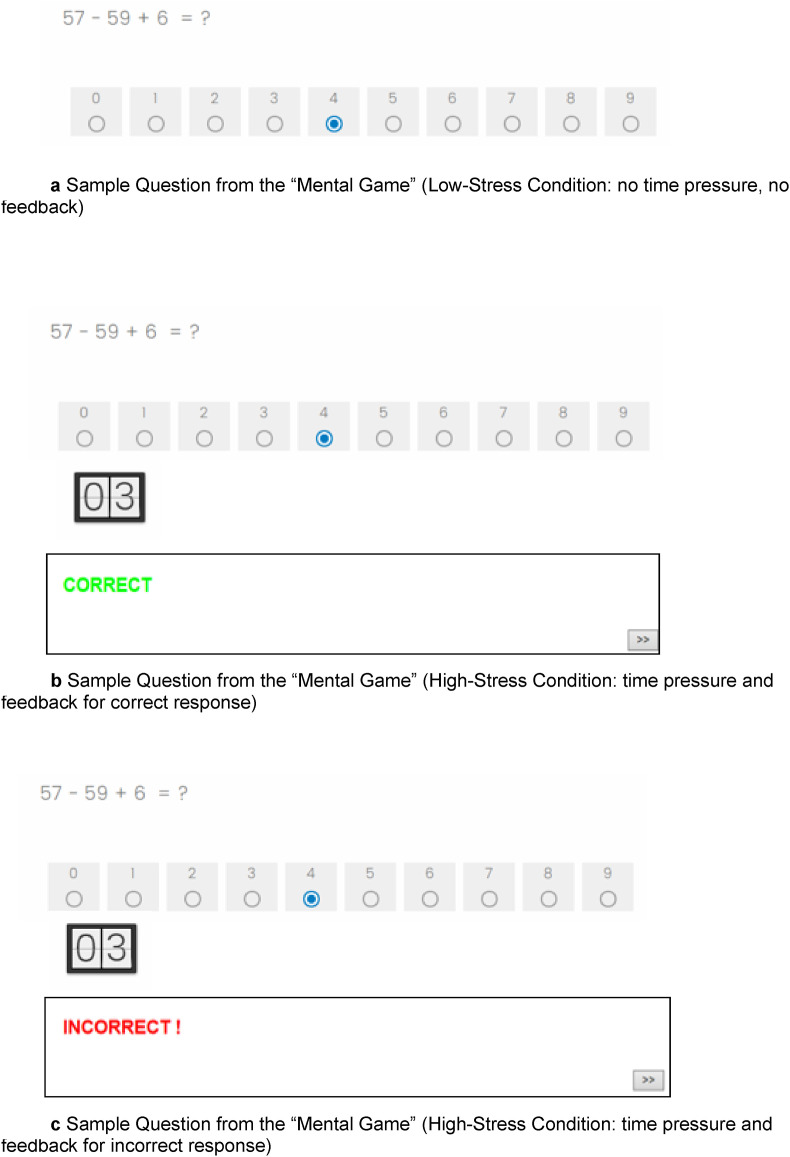
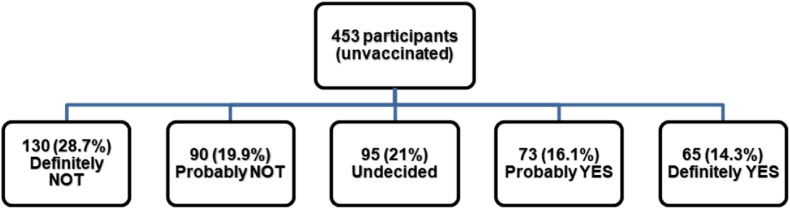
Methods: Two studies were conducted with U.S. residents. Using a cross-sectional design, Study 1 examined the associations between executive function, socio-demographic factors, COVID-19 conspiracy beliefs, trust in health authorities, and COVID-19 vaccine hesitancy. Using an experimental design, Study 2 focused solely on unvaccinated individuals and tested the interactive effect of executive function and stress on willingness to receive a COVID-19 vaccine. We used ordinal logistic regressions to analyze the data.
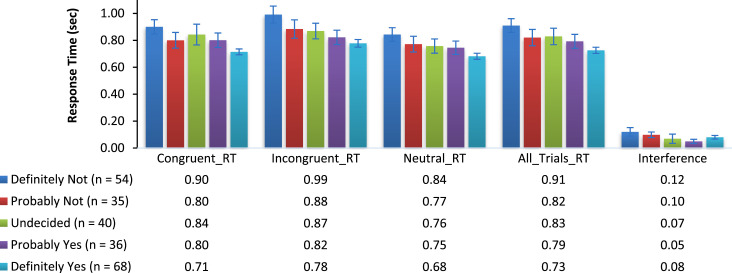
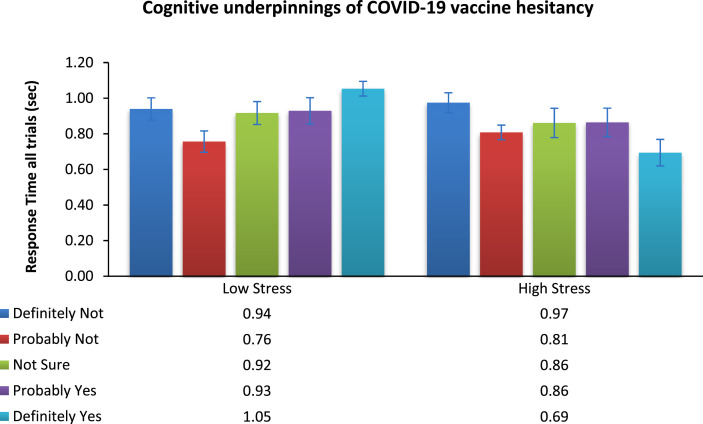
Results: Individual differences in executive function predicted participants' COVID-19 conspiracy beliefs, trust in health authorities, and their willingness to vaccinate against COVID-19. Importantly, the unique contribution of executive function to vaccine hesitancy could not be explained by socio-demographic factors or depressed mood. Furthermore, Study 2 revealed that weaker executive function had detrimental effects on COVID-19 vaccine acceptance and trust in health authorities mainly under heightened stress.
Conclusions: Individual differences in executive function and situational stress jointly impact COVID-19 vaccination decisions and need to be considered together when designing health communications aimed at reducing COVID-19 vaccine hesitancy. Interventions that lower stress and promote trust have the potential to increase vaccine acceptance, especially for individuals with weaker executive function.
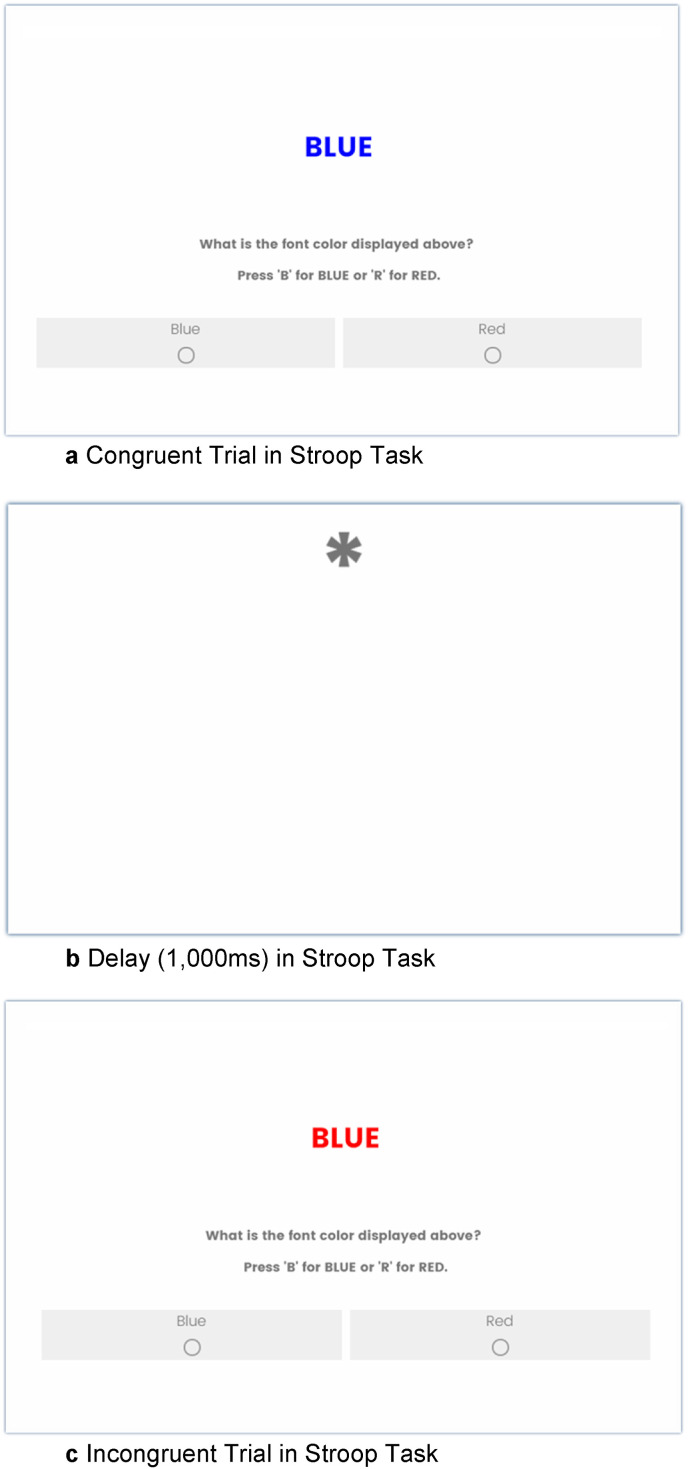
Keywords: COVID-19; Cognition; Executive function; Stress; Stroop task; Trust; Vaccination intentions; Vaccine acceptance; Vaccine hesitancy.
Copyright © 2022. Published by Elsevier Ltd.
Conflict of interest statement
The authors declare no competing interest.
Figures
Similar articles
-
Coronavirus conspiracy suspicions, general vaccine attitudes, trust and coronavirus information source as predictors of vaccine hesitancy among UK residents during the COVID-19 pandemic.Psychol Med. 2023 Jan;53(1):236-247. doi: 10.1017/S0033291721001434. Epub 2021 Apr 12. Psychol Med. 2023. PMID: 33843509 Free PMC article.
-
SARS-CoV-2 variants and the global pandemic challenged by vaccine uptake during the emergence of the Delta variant: A national survey seeking vaccine hesitancy causes.J Infect Public Health. 2022 Jul;15(7):773-780. doi: 10.1016/j.jiph.2022.06.007. Epub 2022 Jun 17. J Infect Public Health. 2022. PMID: 35728424 Free PMC article.
-
COVID-19 Vaccine Hesitancy Among Chinese Population: A Large-Scale National Study.Front Immunol. 2021 Nov 29;12:781161. doi: 10.3389/fimmu.2021.781161. eCollection 2021. Front Immunol. 2021. PMID: 34912346 Free PMC article.
-
Addressing vaccine hesitancy and resistance for COVID-19 vaccines.Int J Nurs Stud. 2022 Jul;131:104241. doi: 10.1016/j.ijnurstu.2022.104241. Epub 2022 Apr 1. Int J Nurs Stud. 2022. PMID: 35489108 Free PMC article. Review.
-
What factors promote vaccine hesitancy or acceptance during pandemics? A systematic review and thematic analysis.Health Promot Int. 2022 Feb 17;37(1):daab105. doi: 10.1093/heapro/daab105. Health Promot Int. 2022. PMID: 34244738
Cited by
-
Cognitive flexibility predicts attitudes towards vaccination: evidence from a New Zealand sample.BMC Psychol. 2024 Oct 14;12(1):550. doi: 10.1186/s40359-024-02048-2. BMC Psychol. 2024. PMID: 39402611 Free PMC article.
-
Understanding attitudes and beliefs regarding COVID-19 vaccines among transitional-aged youth with mental health concerns: a youth-led qualitative study.BMJ Open. 2024 Jan 18;14(1):e080707. doi: 10.1136/bmjopen-2023-080707. BMJ Open. 2024. PMID: 38238177 Free PMC article.
-
What Contributes to COVID-19 Vaccine Hesitancy? A Systematic Review of the Psychological Factors Associated with COVID-19 Vaccine Hesitancy.Vaccines (Basel). 2022 Oct 22;10(11):1777. doi: 10.3390/vaccines10111777. Vaccines (Basel). 2022. PMID: 36366286 Free PMC article. Review.
-
Trauma, adversity, and biological aging: behavioral mechanisms relevant to treatment and theory.Transl Psychiatry. 2024 Jul 12;14(1):285. doi: 10.1038/s41398-024-03004-9. Transl Psychiatry. 2024. PMID: 38997260 Free PMC article. Review.
-
Impact of social media news on COVID-19 vaccine hesitancy and vaccination behavior.Telemat Inform. 2023 May;80:101983. doi: 10.1016/j.tele.2023.101983. Epub 2023 Apr 23. Telemat Inform. 2023. PMID: 37122766 Free PMC article.
References
-
- Buhrmester M., Kwang T., Gosling S.D. Amazon's mechanical Turk: a new source of inexpensive, yet high-quality data? Perspect. Psychol. Sci. 2011;6:3–5. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
