

Entrectinib in children and young adults with solid or primary CNS tumors harboring NTRK, ROS1, or ALK aberrations (STARTRK-NG)
- PMID: 35395680
- PMCID: PMC9527518
- DOI: 10.1093/neuonc/noac087
Entrectinib in children and young adults with solid or primary CNS tumors harboring NTRK, ROS1, or ALK aberrations (STARTRK-NG)
Abstract
Background: Entrectinib is a TRKA/B/C, ROS1, ALK tyrosine kinase inhibitor approved for the treatment of adults and children aged ≥12 years with NTRK fusion-positive solid tumors and adults with ROS1 fusion-positive non-small-cell lung cancer. We report an analysis of the STARTRK-NG trial, investigating the recommended phase 2 dose (RP2D) and activity of entrectinib in pediatric patients with solid tumors including primary central nervous system tumors.
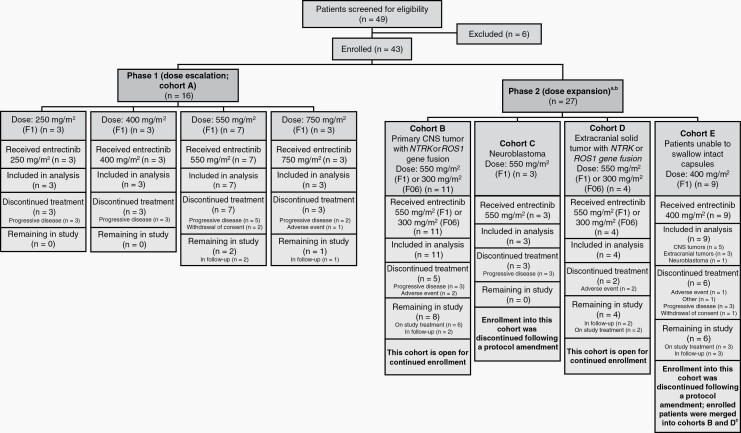
Methods: STARTRK-NG (NCT02650401) is a phase 1/2 trial. Phase 1, dose-escalation of oral, once-daily entrectinib, enrolled patients aged <22 years with solid tumors with/without target NTRK1/2/3, ROS1, or ALK fusions. Phase 2, basket trial at the RP2D, enrolled patients with intracranial or extracranial solid tumors harboring target fusions or neuroblastoma. Primary endpoints: phase 1, RP2D based on toxicity; phase 2, objective response rate (ORR) in patients harboring target fusions. Safety-evaluable patients: ≥1 dose of entrectinib; response-evaluable patients: measurable/evaluable baseline disease and ≥1 dose at RP2D.
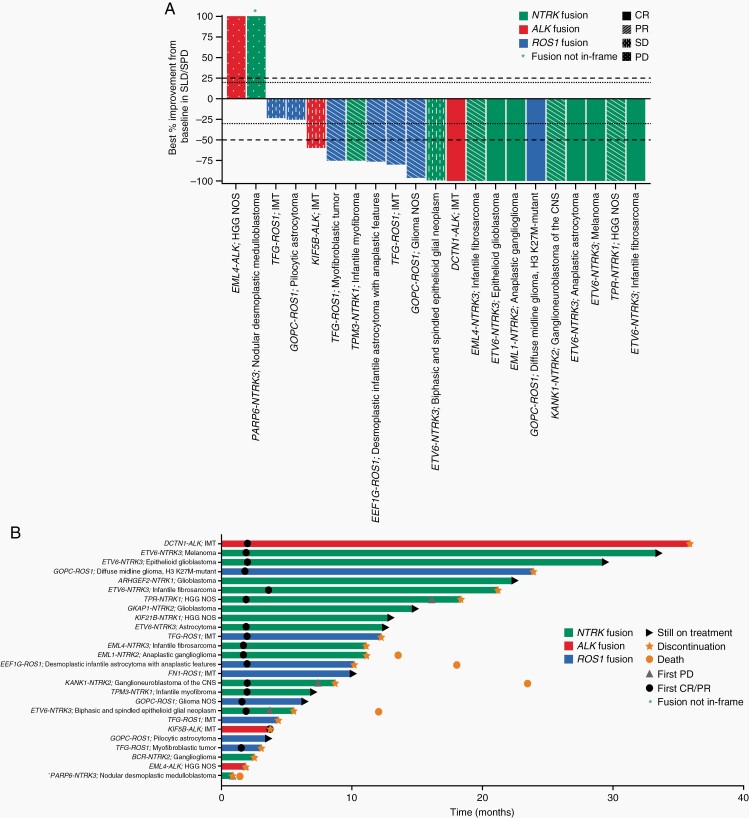
Results: At data cutoff, 43 patients, median age of 7 years, were response-evaluable. In phase 1, 4 patients experienced dose-limiting toxicities. The most common treatment-related adverse event was weight gain (48.8%). Nine patients experienced bone fractures (20.9%). In patients with fusion-positive tumors, ORR was 57.7% (95% CI 36.9-76.7), median duration of response was not reached, and median (interquartile range) duration of treatment was 10.6 months (4.2-18.4).
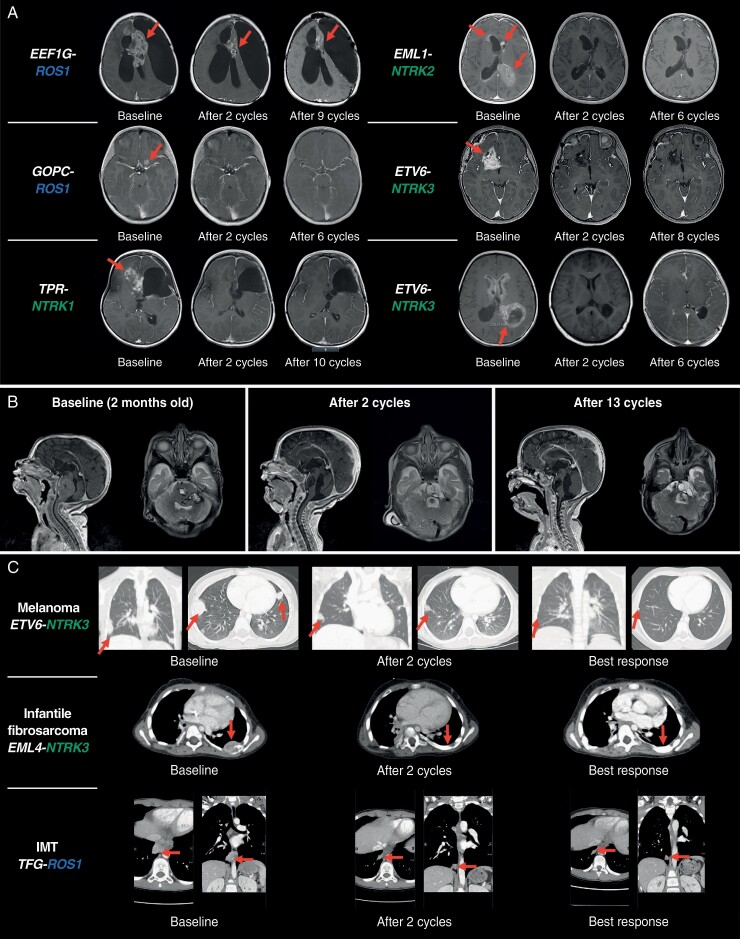
Conclusions: Entrectinib resulted in rapid and durable responses in pediatric patients with solid tumors harboring NTRK1/2/3 or ROS1 fusions.
Keywords: CNS tumors; entrectinib; pediatric; recommended phase 2 dose; solid tumors.
© The Author(s) 2022. Published by Oxford University Press on behalf of the Society for Neuro-Oncology.
Figures
References
-
- Albert CM, Davis JL, Federman N, Casanova M, Laetsch TW. TRK fusion cancers in children: a clinical review and recommendations for screening. J Clin Oncol. 2019;37(6):513–524. - PubMed
