

Scoliosis in dysplastic spondylolisthesis: a clinical survey of 50 young patients
- PMID: 35395763
- PMCID: PMC8991581
- DOI: 10.1186/s12891-022-05297-7
Scoliosis in dysplastic spondylolisthesis: a clinical survey of 50 young patients
Abstract
Background: Dysplastic spondylolisthesis is a rare spinal deformity that occurs mainly in young patients. Although its sagittal parameters had been well stated, coronal abnormalities in these patients were poorly studied. The purposes of this study were: (1) to investigate the prevalence of scoliosis in dysplastic spondylolisthesis;(2) to assess scoliosis resolution or persistence after surgery; and (3) to propose a modified classification of scoliosis associated with dysplastic spondylolisthesis.
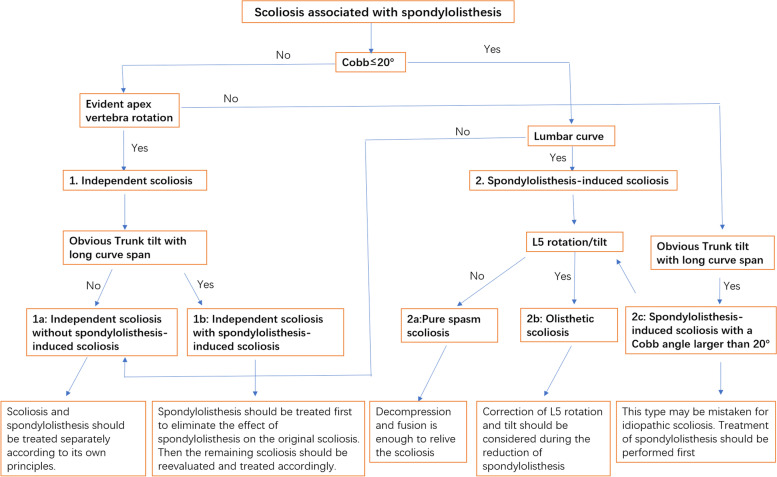
Methods: Fifty patients (average age 14.9 ± 5.6 years) diagnosed with dysplastic spondylolisthesis who underwent surgical treatment were followed up and their data were analyzed. Standing posteroanterior and lateral full spine radiographs were used to measure the coronal and sagittal parameters. Patients with scoliosis, which was defined as a coronal Cobb angle greater than 10°, were divided into three groups according to their curve characteristics: "independent" scoliosis (IS) group, spasm scoliosis (SS) group, and olisthetic scoliosis (OS) group. SS and OS were spondylolisthesis-induced scoliosis. The radiographic parameters and patient-reported outcomes were collected before and after surgery and compared between groups.
Results: The average slip percentage was 62.8% ± 23.1% and the average follow-up time was 51.5 ± 36.4 months (range 3-168 months). Twenty-eight of the 50 (56%) dysplastic spondylolisthesis patients showed scoliosis, of which 8 were IS (24.7° ± 15.2°), 11 were SS (13.9° ± 3.0°), and 9 were OS (12.9° ± 1.9°). By the last follow-up, no scoliosis resolution was observed in the IS group whereas all SS patients were relieved. Of the nine patients with OS, four (44.4%) had scoliosis resolution after surgery.
Conclusion: Distinguishing different types of scoliosis in dysplastic spondylolisthesis patients may help surgeons to plan treatment and understand prognosis. For patients with significant scoliosis, whether "independent" or spondylolisthesis-induced, treatment of spondylolisthesis should be performed first and scoliosis should be observed for a period of time and treated according to the corresponding principles.
Keywords: Adolescent idiopathic scoliosis; Developmental spondylolisthesis; Dysplastic spondylolisthesis; Olisthetic scoliosis; Spasm scoliosis.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures




Similar articles
-
Curve Characteristics and Response of Sciatic and Olisthesis Scoliosis Following L5/S1 Transforaminal Lumbar Interbody Fusion in Adolescent Lumbar Spondylolisthesis.Neurosurgery. 2021 Jan 13;88(2):322-331. doi: 10.1093/neuros/nyaa429. Neurosurgery. 2021. PMID: 33017018
-
Scoliosis research society outcome instrument in evaluation of long-term surgical results in spondylolysis and low-grade isthmic spondylolisthesis in young patients.Spine (Phila Pa 1976). 2005 Feb 1;30(3):336-41. doi: 10.1097/01.brs.0000152375.13316.6a. Spine (Phila Pa 1976). 2005. PMID: 15682016
-
Scoliosis risk factors and outcomes in children with dysplastic spondylolisthesis undergoing surgical reduction and fixation.J Child Orthop. 2023 Jun 24;17(4):360-366. doi: 10.1177/18632521231182430. eCollection 2023 Aug. J Child Orthop. 2023. PMID: 37565003 Free PMC article.
-
Correlation of radiographic, clinical, and patient assessment of shoulder balance following fusion versus nonfusion of the proximal thoracic curve in adolescent idiopathic scoliosis.Spine (Phila Pa 1976). 2002 Sep 15;27(18):2013-20. doi: 10.1097/00007632-200209150-00009. Spine (Phila Pa 1976). 2002. PMID: 12634561 Review.
-
AIS and spondylolisthesis.Eur Spine J. 2013 Mar;22 Suppl 2(Suppl 2):S172-84. doi: 10.1007/s00586-012-2326-8. Epub 2012 May 9. Eur Spine J. 2013. PMID: 22569830 Free PMC article. Review.
References
-
- Rahman RK, Perra J, Weidenbaum M. Wiltse and Marchetti/Bartolozzi classification of spondylolisthesis - guidelines for treatment. In: Bridwell KH, Dewald RL, editors. The Textbook of Spinal Surgery. 3rd. Philadelphia: Lippincott-Wilkins; 2011. pp. 596–562.
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
