

How much preoperative flexion contracture is a predictor for residual flexion contracture after total knee arthroplasty in hemophilic arthropathy and rheumatoid arthritis?
- PMID: 35395934
- PMCID: PMC8994339
- DOI: 10.1186/s43019-022-00146-2
How much preoperative flexion contracture is a predictor for residual flexion contracture after total knee arthroplasty in hemophilic arthropathy and rheumatoid arthritis?
Abstract
Background: Although total knee arthroplasty (TKA) in hemophilic arthropathy (HA) or rheumatoid arthritis (RA) can improve functional ability, the postoperative range of motion (ROM) and prosthesis durability are reduced compared with those in osteoarthritic patients.
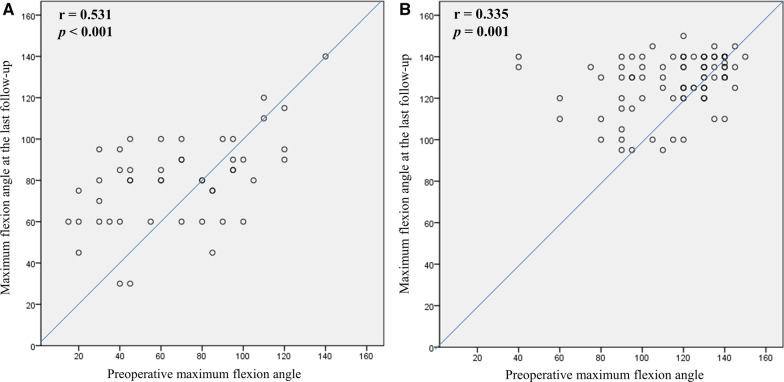
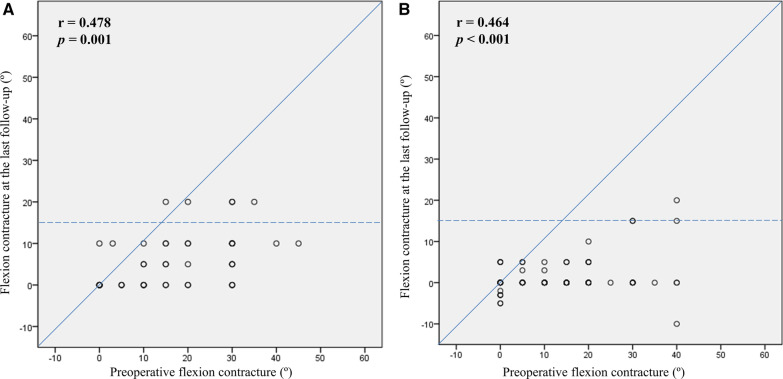
Aim: We aimed to compare (1) the pre- and postoperative flexion contracture after TKA in HA and RA, (2) the threshold of preoperative flexion contracture as a predictor of residual contracture > 15° after TKA, and (3) the survival rate.
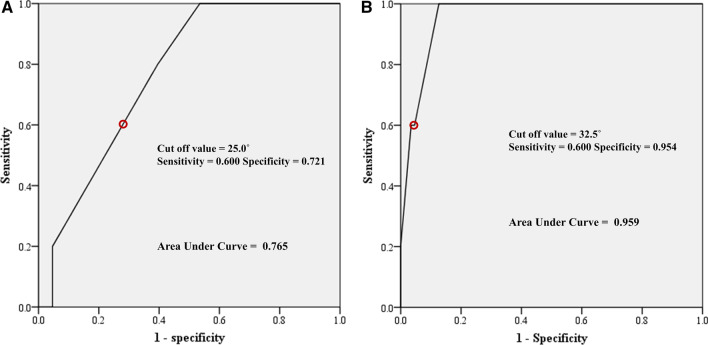
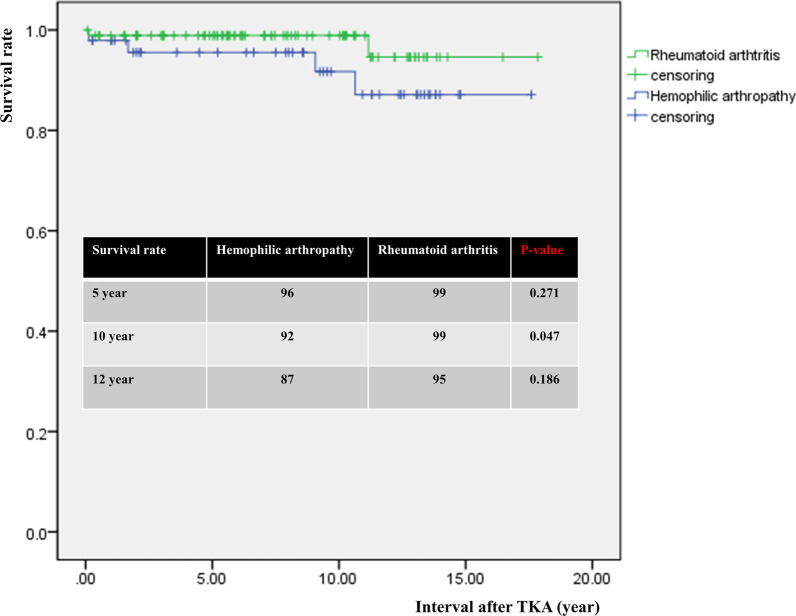
Methods: Data from a consecutive cohort comprising 48 TKAs in HA and 92 TKAs in RA were retrospectively reviewed. The degree of flexion contracture was analyzed. Through receiver operating characteristics analysis, we aimed to determine the cutoff value of preoperative flexion contracture that increases the risk of residual contracture > 15° after TKA and compare the cutoff value in HA and RA. The survival rate was evaluated based on life table analysis and the Kaplan-Meier method.
Results: The degree of preoperative flexion contracture was not significantly different. The degree of postoperative residual flexion contracture was 5.6° in the HA group and 1.4° in the RA group, respectively (p < 0.001). The cutoff value of preoperative flexion contracture for residual contracture of > 15° at last-follow up was 25.0° in the HA group and 32.5° in the RA group. The 5- and 12-year survival rates were 96% and 87% in the HA and 99% and 95% in the RA group, respectively (n.s.).
Conclusions: The postoperative residual flexion contracture was greater and the cutoff value of preoperative flexion contracture for residual contracture was smaller in the HA group than the RA group. Appropriate intra- and postoperative care to avoid postoperative residual contracture is required in HA patients.
Level of evidence: III.
Keywords: Arthroplasty; Complications; Flexion contracture; Hemophilia; Knee; Rheumatoid arthritis.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

Similar articles
-
Predictors of Recurrent Flexion Contracture after Total Knee Arthroplasty in Osteoarthritic Knees with Greater Than 15° Flexion Contracture.Clin Orthop Surg. 2023 Oct;15(5):770-780. doi: 10.4055/cios22207. Epub 2022 Nov 22. Clin Orthop Surg. 2023. PMID: 37811511 Free PMC article.
-
[Balancing of soft tissues in total knee arthroplasty for patients with rheumatoid arthritis with knee flexion contracture].Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2008 Oct;22(10):1173-6. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2008. PMID: 18979871 Chinese.
-
Pre-operative flexion contracture determines the functional outcome of haemophilic arthropathy treated with total knee arthroplasty.Haemophilia. 2012 May;18(3):358-63. doi: 10.1111/j.1365-2516.2011.02695.x. Epub 2011 Nov 21. Haemophilia. 2012. PMID: 22103453
-
Mid-term outcomes and complications of total knee arthroplasty in haemophilic arthropathy: A review of consecutive 131 knees between 2006 and 2015 in a single institute.Haemophilia. 2018 Mar;24(2):299-306. doi: 10.1111/hae.13383. Epub 2017 Nov 29. Haemophilia. 2018. PMID: 29193440 Review.
-
Total Knee Arthroplasty in Patients with Hemophilia: What Do We Know?Arch Bone Jt Surg. 2020 Jul;8(4):470-478. doi: 10.22038/abjs.2019.42247.2149. Arch Bone Jt Surg. 2020. PMID: 32884968 Free PMC article. Review.
Cited by
-
Predictors of Recurrent Flexion Contracture after Total Knee Arthroplasty in Osteoarthritic Knees with Greater Than 15° Flexion Contracture.Clin Orthop Surg. 2023 Oct;15(5):770-780. doi: 10.4055/cios22207. Epub 2022 Nov 22. Clin Orthop Surg. 2023. PMID: 37811511 Free PMC article.
-
Comparison of Clinical and Radiographic Outcomes According to the Presence or Absence of a Posterior Draw Force during Graft Fixation in Anterior Cruciate Ligament Reconstruction.Medicina (Kaunas). 2022 Dec 5;58(12):1787. doi: 10.3390/medicina58121787. Medicina (Kaunas). 2022. PMID: 36556989 Free PMC article.
-
The effect of HIV prevalence, CD4 counts and disease severity on the outcome of total knee arthroplasty for haemophilic arthropathy: a systematic review and meta-analysis.Eur J Orthop Surg Traumatol. 2023 Dec;33(8):3235-3254. doi: 10.1007/s00590-023-03586-y. Epub 2023 May 22. Eur J Orthop Surg Traumatol. 2023. PMID: 37212914
-
Femoral Tunnel Position Affects Postoperative Femoral Tunnel Widening after Anterior Cruciate Ligament Reconstruction with Tibialis Anterior Allograft.J Clin Med. 2023 Mar 2;12(5):1966. doi: 10.3390/jcm12051966. J Clin Med. 2023. PMID: 36902753 Free PMC article.
-
Complications and Implant Survival of Total Knee Arthroplasty in People with Hemophilia.J Clin Med. 2022 Oct 23;11(21):6244. doi: 10.3390/jcm11216244. J Clin Med. 2022. PMID: 36362472 Free PMC article. Review.
References
-
- Chang MJ, Kang SB, Chang CB, et al. Posterior condylar offset changes and its effect on clinical outcomes after posterior-substituting, fixed-bearing total knee arthroplasty: anterior versus posterior referencing. Knee Surg Relat Res. 2020;32(1):10. doi: 10.1186/s43019-019-0022-2. - DOI - PMC - PubMed
-
- Hoots WK. Seminars in hematology. Amsterdam: Elsevier; 2006. Pathogenesis of hemophilic arthropathy; pp. S18–S22. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
