

Characteristics of the patellofemoral joint of patients with DDH and the effects of Bernese periacetabular osteotomy on the patellofemoral joint
- PMID: 35395939
- PMCID: PMC8991590
- DOI: 10.1186/s12891-022-05291-z
Characteristics of the patellofemoral joint of patients with DDH and the effects of Bernese periacetabular osteotomy on the patellofemoral joint
Abstract
Background: Some patients with developmental dysplasia of the hip (DDH) complained of anterior knee pain (AKP) before and after Bernese periacetabular osteotomy (PAO) surgery. The purpose of this study was to (1) identify the characteristics of patellofemoral joint (PFJ) deformities in patients with DDH and (2) to determine the effects of PAO on the PFJ.
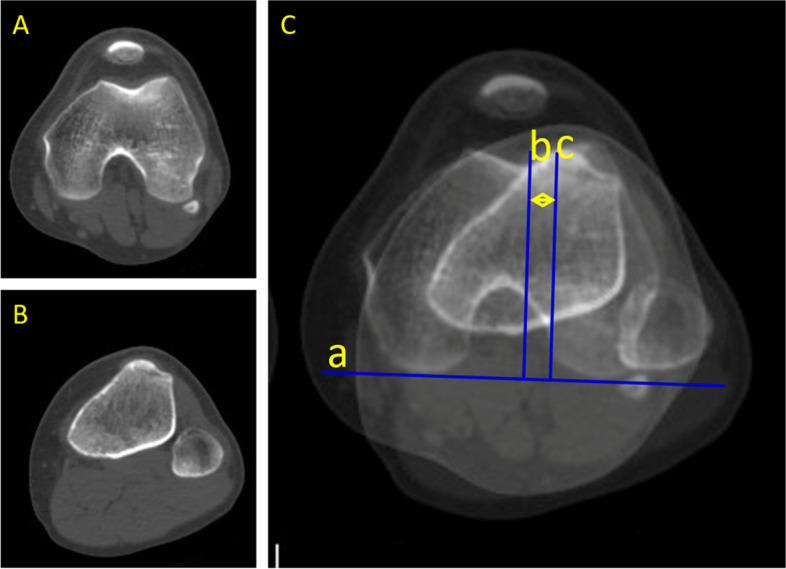
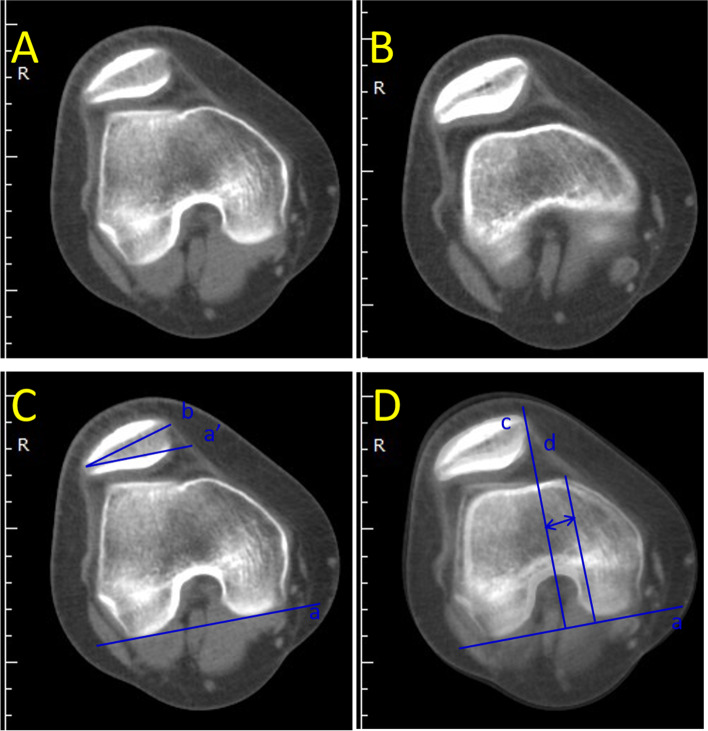
Methods: Seventy patients (86 hips) were included in the DDH group. Thirty-three patients (33 knees) without AKP and hip pain were included in the control group. All patients underwent simultaneous CT scans of the hip and knee joints before PAO and after hardware removal surgery. The distance from the anterior inferior iliac spine to the ilioischial line (DAI), was measured in DDH patients. Imaging parameters of knees, including the sulcus angle (SA), femoral trochlear depth (FTD), patellar width (PW), tibial tuberosity-trochlear groove (TT-TG), patellar tilt angle (PTA) and lateral shift of the patella (LSP) were measured in patients in both the DDH and control group. TT-TG, PTA, and LSP of DDH patients were measured before PAO and after hardware removal. The DAI, PTA, LSP and TT-TG of all DDH patients before and after Bernese PAO were compared using paired t-tests. The FTD, PW, and SA of the DDH patients and the control group were analyzed using independent t-tests. PTA, TT-TG, and LSP between the control group and preoperative DDH patients, between the control group and post PAO patients were compared using independent t-tests.
Results: The DAI changed from 4.04 ± 0.61 mm before PAO surgery to 5.44 ± 0.63 mm after PAO surgery. The SA of the DDH group (140.69 ± 11.30 degree) was greater than that of the control group (130.82 ± 6.43 degree). The FTD and the PW of the DDH group (5.45 ± 1.59 mm, 4.16 ± 0.36 mm) were smaller than that of the control group (7.39 ± 1.20 mm, 4.24 ± 0.38 mm). The changes in LSP, PTA, and TT-TG before and after surgery were not statistically significant. Both before and after PAO, there was no statistically significant difference in the parameters of LSP, PTA, and TT-TG compared with the control group.
Conclusion: The knee joints of DDH patients presented a certain degree of femur trochlear groove dysplasia and patellofemoral instability. PAO surgery did not change PFJ stability, although the origination point of the rectus femoris muscle moved laterally during PAO surgery.
Keywords: Anterior knee pain; Bernese periacetabular osteotomy; Developmental dysplasia of the hip; Patellofemoral joint.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures


Similar articles
-
Correlation of radiographic patellofemoral indices with tibial tubercle transfer distance in Fulkerson osteotomy procedures.Iowa Orthop J. 2014;34:24-9. Iowa Orthop J. 2014. PMID: 25328455 Free PMC article.
-
Varus inclination of the tibia is related to patellofemoral osteoarthritis in Japanese female patients with moderate knee osteoarthritis.Knee Surg Sports Traumatol Arthrosc. 2021 Feb;29(2):652-658. doi: 10.1007/s00167-020-06000-w. Epub 2020 Apr 21. Knee Surg Sports Traumatol Arthrosc. 2021. PMID: 32318752
-
Hybrid high tibial osteotomy is superior to medial opening high tibial osteotomy for the treatment of varus knee with patellofemoral osteoarthritis.Knee Surg Sports Traumatol Arthrosc. 2019 Apr;27(4):1332-1338. doi: 10.1007/s00167-018-5015-2. Epub 2018 Jun 8. Knee Surg Sports Traumatol Arthrosc. 2019. PMID: 29947840
-
Osteoarthritic knees have a highly variable patellofemoral alignment: a systematic review.Knee Surg Sports Traumatol Arthrosc. 2021 Feb;29(2):483-490. doi: 10.1007/s00167-020-05928-3. Epub 2020 Mar 12. Knee Surg Sports Traumatol Arthrosc. 2021. PMID: 32162047
-
Healthy knees have a highly variable patellofemoral alignment: a systematic review.Knee Surg Sports Traumatol Arthrosc. 2020 Feb;28(2):398-406. doi: 10.1007/s00167-019-05587-z. Epub 2019 Jun 29. Knee Surg Sports Traumatol Arthrosc. 2020. PMID: 31256215
Cited by
-
Medial patellofemoral ligament reconstruction combined with derotational distal femoral osteotomy yields better outcomes than isolated procedures in patellar dislocation with increased femoral anteversion.Knee Surg Sports Traumatol Arthrosc. 2023 Jul;31(7):2888-2896. doi: 10.1007/s00167-022-07264-0. Epub 2022 Dec 1. Knee Surg Sports Traumatol Arthrosc. 2023. PMID: 36454293
-
Knee morphology and patella malalignment in neglected developmental dysplasia of the hip: a systematic review and meta-analysis.J Orthop Surg Res. 2025 May 20;20(1):489. doi: 10.1186/s13018-025-05877-y. J Orthop Surg Res. 2025. PMID: 40394669 Free PMC article.
References
-
- Ganz R, et al. A new periacetabular osteotomy for the treatment of hip dysplasias. Technique and preliminary results. Clin Orthop Relat Res. 1988;232:26–36. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
