

Results of the COMPARE trial of Constraint-induced or Multimodality Aphasia Therapy compared with usual care in chronic post-stroke aphasia
- PMID: 35396340
- PMCID: PMC9148985
- DOI: 10.1136/jnnp-2021-328422
Results of the COMPARE trial of Constraint-induced or Multimodality Aphasia Therapy compared with usual care in chronic post-stroke aphasia
Abstract
Background: While meta-analyses confirm treatment for chronic post-stroke aphasia is effective, a lack of comparative evidence for different interventions limits prescription accuracy. We investigated whether Constraint-Induced Aphasia Therapy Plus (CIAT-plus) and/or Multimodality Aphasia Therapy (M-MAT) provided greater therapeutic benefit compared with usual community care and were differentially effective according to baseline aphasia severity.
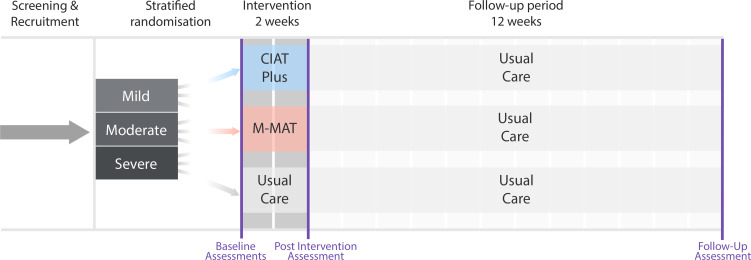
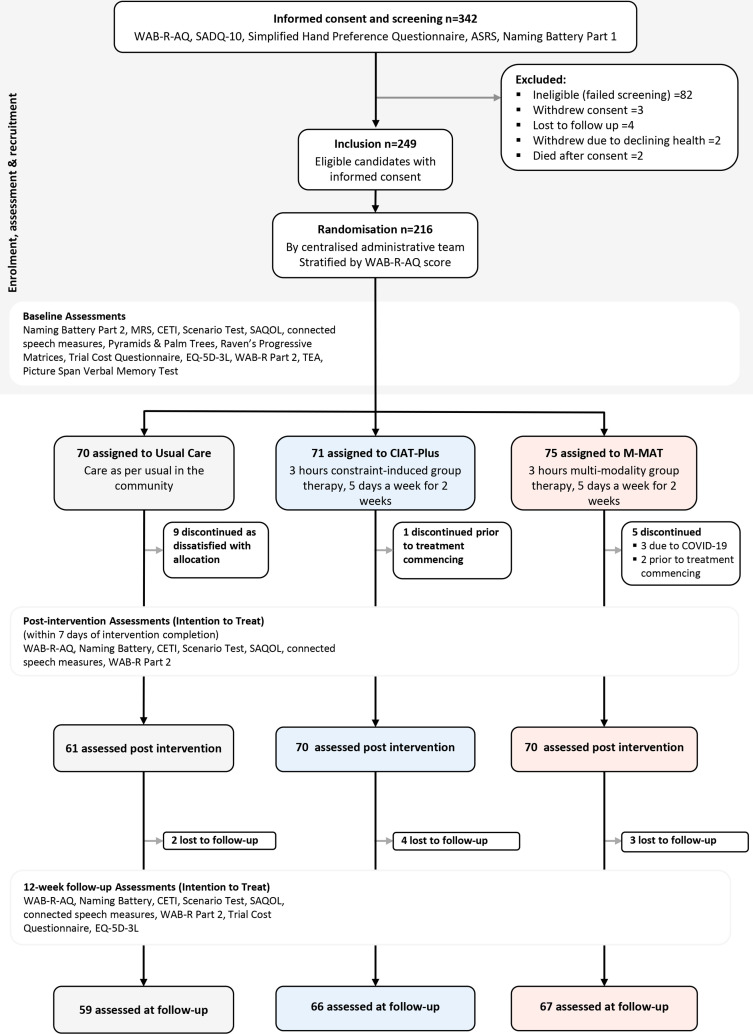
Methods: We conducted a three-arm, multicentre, parallel group, open-label, blinded endpoint, phase III, randomised-controlled trial. We stratified eligible participants by baseline aphasia on the Western Aphasia Battery-Revised Aphasia Quotient (WAB-R-AQ). Groups of three participants were randomly assigned (1:1:1) to 30 hours of CIAT-Plus or M-MAT or to usual care (UC). Primary outcome was change in aphasia severity (WAB-R-AQ) from baseline to therapy completion analysed in the intention-to-treat population. Secondary outcomes included word retrieval, connected speech, functional communication, multimodal communication, quality of life and costs.
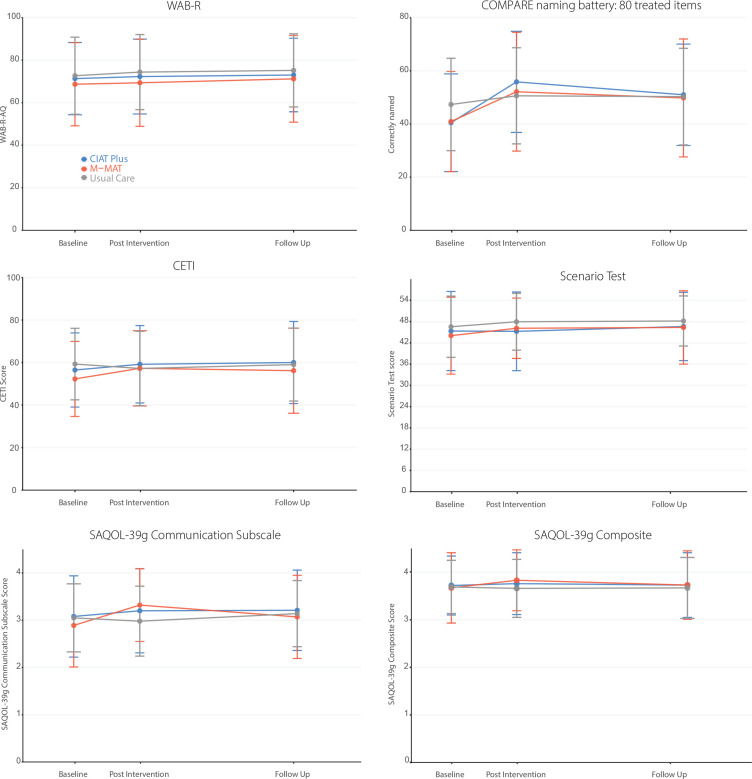
Results: We analysed 201 participants (70 in CIAT-Plus, 70 in M-MAT and 61 in UC). Aphasia severity was not significantly different between groups at postintervention: 1.05 points (95% CI -0.78 to 2.88; p=0.36) UC group vs CIAT-Plus; 1.06 points (95% CI -0.78 to 2.89; p=0.36) UC group vs M-MAT; 0.004 points (95% CI -1.76 to 1.77; p=1.00) CIAT-Plus vs M-MAT. Word retrieval, functional communication and communication-related quality of life were significantly improved following CIAT-Plus and M-MAT. Word retrieval benefits were maintained at 12-week follow-up.
Conclusions: CIAT-Plus and M-MAT were effective for word retrieval, functional communication, and quality of life, while UC was not. Future studies should explore predictive characteristics of responders and impacts of maintenance doses.
Trial registration number: ACTRN 2615000618550.
Keywords: aphasia; randomised trials; rehabilitation; stroke.
© Author(s) (or their employer(s)) 2022. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: MLR, LN, DC, LT, EG, MM, TR, DAC, JK and MH were members of the COMPARE steering committee, chaired by MLR.
Figures
References
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical