

Update of endoscopic classification system of adenoid hypertrophy based on clinical experience on 7621 children
- PMID: 35396589
- PMCID: PMC9330757
- DOI: 10.14639/0392-100X-N1832
Update of endoscopic classification system of adenoid hypertrophy based on clinical experience on 7621 children
Abstract
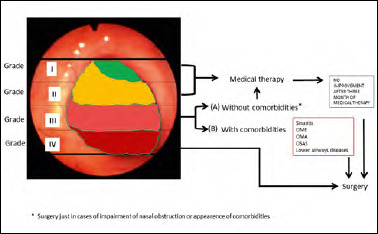
Introduction: Nasal endoscopy is likely to be the method of choice to evaluate nasal obstruction and adenoid hypertrophy (AH) in children given its excellent diagnostic accuracy and low risk for the patient. The aim of this study was to update the previous classification of AH to guide physicians in choosing the best therapeutic option.
Materials and methods: This is a retrospective observational study including 7621 children (3565 females; mean age 5.92; range: 3-14 years) who were managed for adenoid hypertrophy at our institution between 2003 and 2018. All patients were initially treated with medical therapy and then with surgery if not adequately controlled. We performed a specific analysis based on the presence or absence of comorbidities.
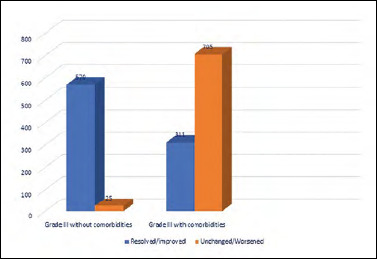
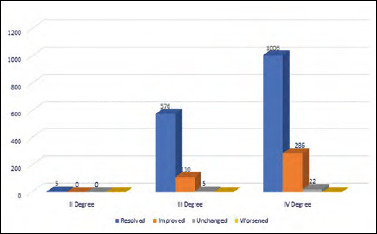
Results: In 1845 (24.21%) patients, adenoid obstruction was classified as Grade I when the fiberoptic endoscopy showed adenoid tissue occupying < 25% of choanal space. In 2829 of 7621 (37.12%) patients, the adenoid tissue was scored as Grade II since it was confined to the upper half of nasopharynx, with sufficiently pervious choana and visualisation of tube ostium. In 1611 of 7621 (21.14%) cases, adenoid vegetation occupied about 75% of the nasopharynx with partial involvement of tube ostium and considerable obstruction of choanal openings, and was classified as Grade III. Finally, 1336 of 7621 (17.53%) patients were scored as Grade IV due to complete obstruction with adenoid tissue reaching the lower choanal border without allowing the visualisation of the tube ostium. Based on resolution of symptoms in Grade III obstruction after medical therapy (that was mostly seen in patients without comorbidities), we divided patients in two subclasses: Grade IIIA was not associated with comorbidities, while Grade IIIB was correlated with important comorbidities.
Conclusions: These results can be useful to guide medical or surgical therapeutic intervention. In patients with class IIIB AH, surgical treatment offered adequate control not only of nasal symptoms but also of associated comorbidities.
Aggiornamento del sistema di classificazione endoscopica dell’ipertrofia adenoidea basato sulla nostra esperienza clinica su 7621 bambini.
Introduzione: L’endoscopia nasale è probabilmente il metodo di scelta per valutare l’ostruzione nasale e l’ipertrofia adenoidea (IA) nei bambini, poiché ha un’eccellente accuratezza diagnostica e un basso rischio per il paziente. Lo scopo di questo studio è di aggiornare la precedente classificazione di IA per guidare i medici a scegliere la migliore opzione terapeutica.
Materiali e metodi: Questo è uno studio osservazionale retrospettivo che include 7621 bambini (3565 femmine; età media 5,92; range: 3-14 anni) che sono stati seguiti per l’ipertrofia adenoidea presso il nostro istituto tra il 2003 e il 2018. Tutti i pazienti sono stati inizialmente trattati con terapia medica e successivamente con terapia chirurgica, se non adeguatamente controllati. Un’analisi specifica è stata condotta sulla base delle comorbidità.
Risultati: In 1845 pazienti (24,21%) l’immagine dell’endoscopia a fibre ottiche evidenziava uno scarso tessuto adenoideo occupante < 25% delle aperture coanale: ostruzione adenoidea di Grado I. In 2829/7621 (37,12%) il tessuto adenoideo era confinato alla metà superiore del rinofaringe, con coana sufficientemente pervia e visualizzazione dell’ostio tubarico: Grado II. In 1611/7621 (21,14%), la vegetazione adenoidea occupava circa il 75% del rinofaringe, con parziale coinvolgimento dell’ostio tubarico e notevole ostruzione delle aperture coanali: Grado III. In 1336/7621 (17,53%) l’ostruzione era quasi completa e il tessuto adenoideo raggiungeva il bordo inferiore della coana senza consentire la visualizzazione dell’ostio tubarico: Grado IV. Sulla base della risoluzione dei sintomi nell’ostruzione di Grado III dopo terapia medica (che è stata evidenziata principalmente nei pazienti senza comorbidità), abbiamo diviso i pazienti in due sottoclassi: il Grado IIIA non era associato a comorbidità, mentre il Grado IIIB era correlato a comorbidità importanti.
Conclusioni: I nostri risultati possono essere utili per indicare un intervento terapeutico medico o chirurgico. Essi dimostrano che nei pazienti di Grado IIIB, il trattamento chirurgico offre un buon controllo non solo dei sintomi nasali, ma anche delle principali comorbidità.
Keywords: adenoid hypertrophy; classification; nasal endoscopy.
Copyright © 2022 Società Italiana di Otorinolaringoiatria e Chirurgia Cervico-Facciale, Rome, Italy.
Figures
References
-
- Major MP, Saltaji H, El-Hakim H, et al. The accuracy of diagnostic tests for adenoid hypertrophy: a systematic review. J Am Dent Assoc 2014;145:247-254. https://doi.org/10.14219/jada.2013.31 10.14219/jada.2013.31 - DOI - PubMed
-
- Chandra RK, Patadia MO, Raviv J. Diagnosis of nasal airway obstruction. Otolaryngol Clin North Am 2009;42:207-225. https://doi.org/10.1016/j.otc.2009.01.004 10.1016/j.otc.2009.01.004 - DOI - PubMed
-
- Marchisio P, Torretta S, Capaccio P, et al. Clinical assessment of adenoidal obstruction based on the nasal obstruction index is no longer useful in children. Otolaryngol Head Neck Surg 2010;142:237-241. https://doi.org/10.1016/j.otohns.2009.10.027 10.1016/j.otohns.2009.10.027 - DOI - PubMed
-
- Ysunza A, Pamplona MC, Quiroz J, et al. Maxillary growth in patients with complete cleft lip and palate, operated on around 4-6 months of age. Int J Pediatr Otorhinolaryngol 2010;74:482-485. https://doi.org/10.1016/j.ijporl.2010.01.024 10.1016/j.ijporl.2010.01.024 - DOI - PubMed
-
- Ysunza A, Pamplona MC, Ortega JM, et al. Video fluoroscopy for evaluating adenoid hypertrophy in children. Int J Pediatr Otorhinolaryngol 2008;72:1159-1165. https://doi.org/10.1016/j.ijporl.2008.03.022 10.1016/j.ijporl.2008.03.022 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
