

Risk factors and prognostic implications of diagnosis of cancer within 30 days after an emergency hospital admission (emergency presentation): an International Cancer Benchmarking Partnership (ICBP) population-based study
- PMID: 35397210
- PMCID: PMC9046095
- DOI: 10.1016/S1470-2045(22)00127-9
Risk factors and prognostic implications of diagnosis of cancer within 30 days after an emergency hospital admission (emergency presentation): an International Cancer Benchmarking Partnership (ICBP) population-based study
Abstract
Background: Greater understanding of international cancer survival differences is needed. We aimed to identify predictors and consequences of cancer diagnosis through emergency presentation in different international jurisdictions in six high-income countries.
Methods: Using a federated analysis model, in this cross-sectional population-based study, we analysed cancer registration and linked hospital admissions data from 14 jurisdictions in six countries (Australia, Canada, Denmark, New Zealand, Norway, and the UK), including patients with primary diagnosis of invasive oesophageal, stomach, colon, rectal, liver, pancreatic, lung, or ovarian cancer during study periods from Jan 1, 2012, to Dec 31, 2017. Data were collected on cancer site, age group, sex, year of diagnosis, and stage at diagnosis. Emergency presentation was defined as diagnosis of cancer within 30 days after an emergency hospital admission. Using logistic regression, we examined variables associated with emergency presentation and associations between emergency presentation and short-term mortality. We meta-analysed estimates across jurisdictions and explored jurisdiction-level associations between cancer survival and the percentage of patients diagnosed as emergencies.
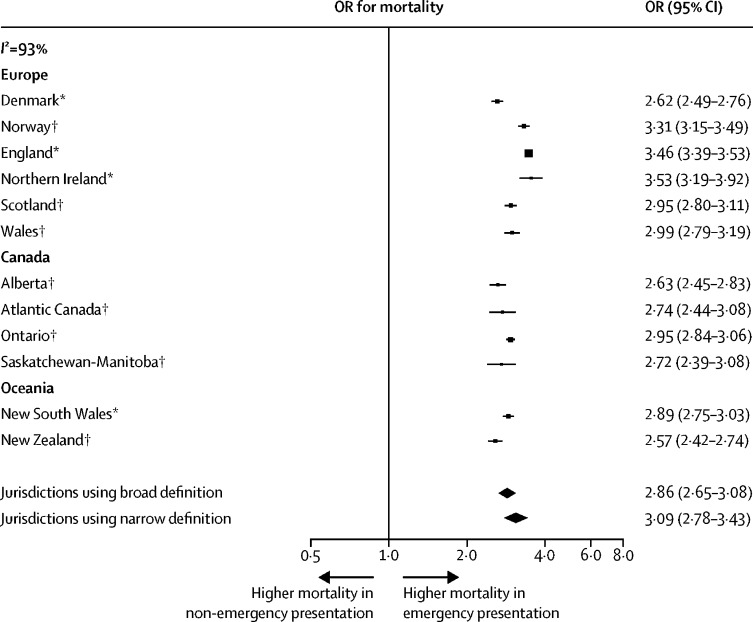
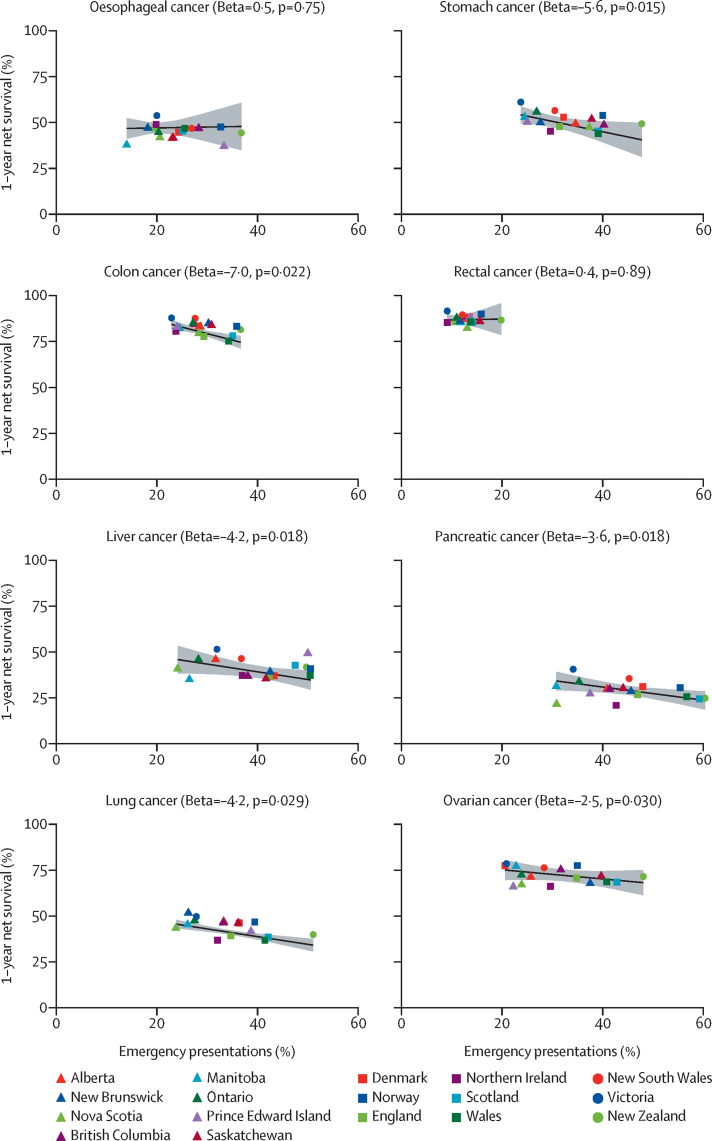
Findings: In 857 068 patients across 14 jurisdictions, considering all of the eight cancer sites together, the percentage of diagnoses through emergency presentation ranged from 24·0% (9165 of 38 212 patients) to 42·5% (12 238 of 28 794 patients). There was consistently large variation in the percentage of emergency presentations by cancer site across jurisdictions. Pancreatic cancer diagnoses had the highest percentage of emergency presentations on average overall (46·1% [30 972 of 67 173 patients]), with the jurisdictional range being 34·1% (1083 of 3172 patients) to 60·4% (1317 of 2182 patients). Rectal cancer had the lowest percentage of emergency presentations on average overall (12·1% [10 051 of 83 325 patients]), with a jurisdictional range of 9·1% (403 of 4438 patients) to 19·8% (643 of 3247 patients). Across the jurisdictions, older age (ie, 75-84 years and 85 years or older, compared with younger patients) and advanced stage at diagnosis compared with non-advanced stage were consistently associated with increased emergency presentation risk, with the percentage of emergency presentations being highest in the oldest age group (85 years or older) for 110 (98%) of 112 jurisdiction-cancer site strata, and in the most advanced (distant spread) stage category for 98 (97%) of 101 jurisdiction-cancer site strata with available information. Across the jurisdictions, and despite heterogeneity in association size (I2=93%), emergency presenters consistently had substantially greater risk of 12-month mortality than non-emergency presenters (odds ratio >1·9 for 112 [100%] of 112 jurisdiction-cancer site strata, with the minimum lower bound of the related 95% CIs being 1·26). There were negative associations between jurisdiction-level percentage of emergency presentations and jurisdiction-level 1-year survival for colon, stomach, lung, liver, pancreatic, and ovarian cancer, with a 10% increase in percentage of emergency presentations in a jurisdiction being associated with a decrease in 1-year net survival of between 2·5% (95% CI 0·28-4·7) and 7·0% (1·2-13·0).
Interpretation: Internationally, notable proportions of patients with cancer are diagnosed through emergency presentation. Specific types of cancer, older age, and advanced stage at diagnosis are consistently associated with an increased risk of emergency presentation, which strongly predicts worse prognosis and probably contributes to international differences in cancer survival. Monitoring emergency presentations, and identifying and acting on contributing behavioural and health-care factors, is a global priority for cancer control.
Funding: Canadian Partnership Against Cancer; Cancer Council Victoria; Cancer Institute New South Wales; Cancer Research UK; Danish Cancer Society; National Cancer Registry Ireland; The Cancer Society of New Zealand; National Health Service England; Norwegian Cancer Society; Public Health Agency Northern Ireland, on behalf of the Northern Ireland Cancer Registry; the Scottish Government; Western Australia Department of Health; and Wales Cancer Network.
Copyright © 2022 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declarations of interests OB and GM declare salary compensation for analysis of trial data in preparation for review by the Data Safety Monitoring Board for the POWERRANGER trial (NCT01404156), unrelated to this project. BD declares project funding from the Velux Foundation (Velux Fonden) and the Nordic Collaboration Cancer Care Pathways, for the Danish Cancer Society. ATG reports support to her employer (Queen's University Belfast) from the Public Health Agency for Northern Ireland. DWD declares support to his employer (Northern Ireland Cancer Registry) from the Public Health Agency for Northern Ireland. DWH declares project support from Public Health Wales NHS Trust and Macmillan Cancer Support, and personal payment for research consultancy fees from Pfizer for work done by Swansea University concerning value-based health care, unrelated to this work. CGCAJ declares past part-employment by the Cancer Society of New Zealand, who co-sponsors the project. HJ declares research grant funding from the Velux Foundation (Velux Fonden). BM and YN declare research grant funding to the Cancer Registry of Norway from the Norwegian Cancer Society. RST declares project support to Public Health Wales NHS Trust from the NHS Wales Cancer Network and Macmillan Cancer Support. RRW reports research grant funding from the Michael Smith Foundation for Health Research, and the First Nations Health Authority and Canadian Partnership Against Cancer. GL declares research grant funding from the study sponsors to his employer (University College London).
Figures
References
-
- De Angelis R, Sant M, Coleman MP, et al. Cancer survival in Europe 1999–2007 by country and age: results of EUROCARE–5-a population-based study. Lancet Oncol. 2014;15:23–34. - PubMed
-
- Zhou Y, Abel GA, Hamilton W, et al. Diagnosis of cancer as an emergency: a critical review of current evidence. Nat Rev Clin Oncol. 2017;14:45–56. - PubMed
-
- Pham TM, Gomez-Cano M, Salika T, Jardel D, Abel GA, Lyratzopoulos G. Diagnostic route is associated with care satisfaction independently of tumour stage: evidence from linked English Cancer Patient Experience Survey and cancer registration data. Cancer Epidemiol. 2019;61:70–78. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
