Assessing the aneurysm occlusion efficacy of a shear-thinning biomaterial in a 3D-printed model
- PMID: 35397405
- PMCID: PMC9060636
- DOI: 10.1016/j.jmbbm.2022.105156
Assessing the aneurysm occlusion efficacy of a shear-thinning biomaterial in a 3D-printed model
Abstract
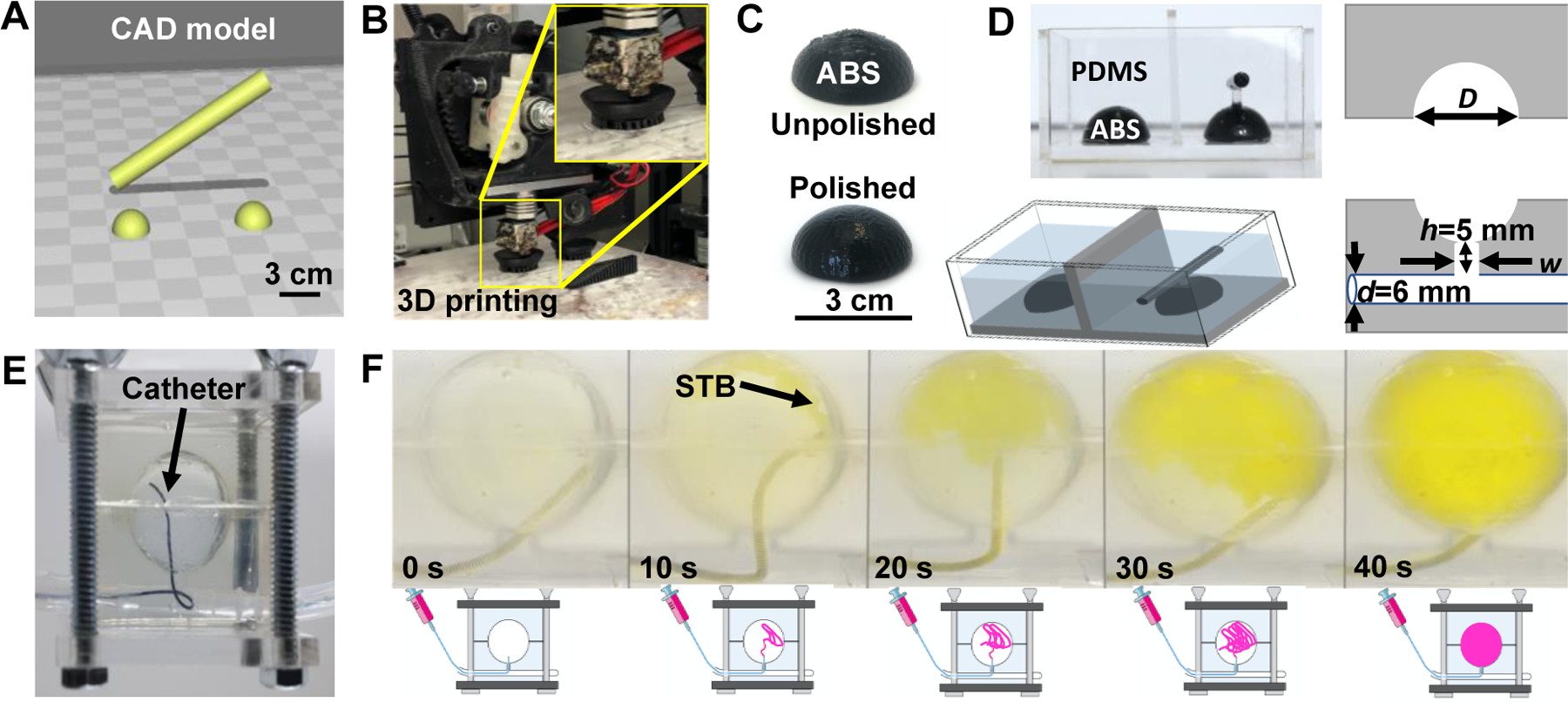
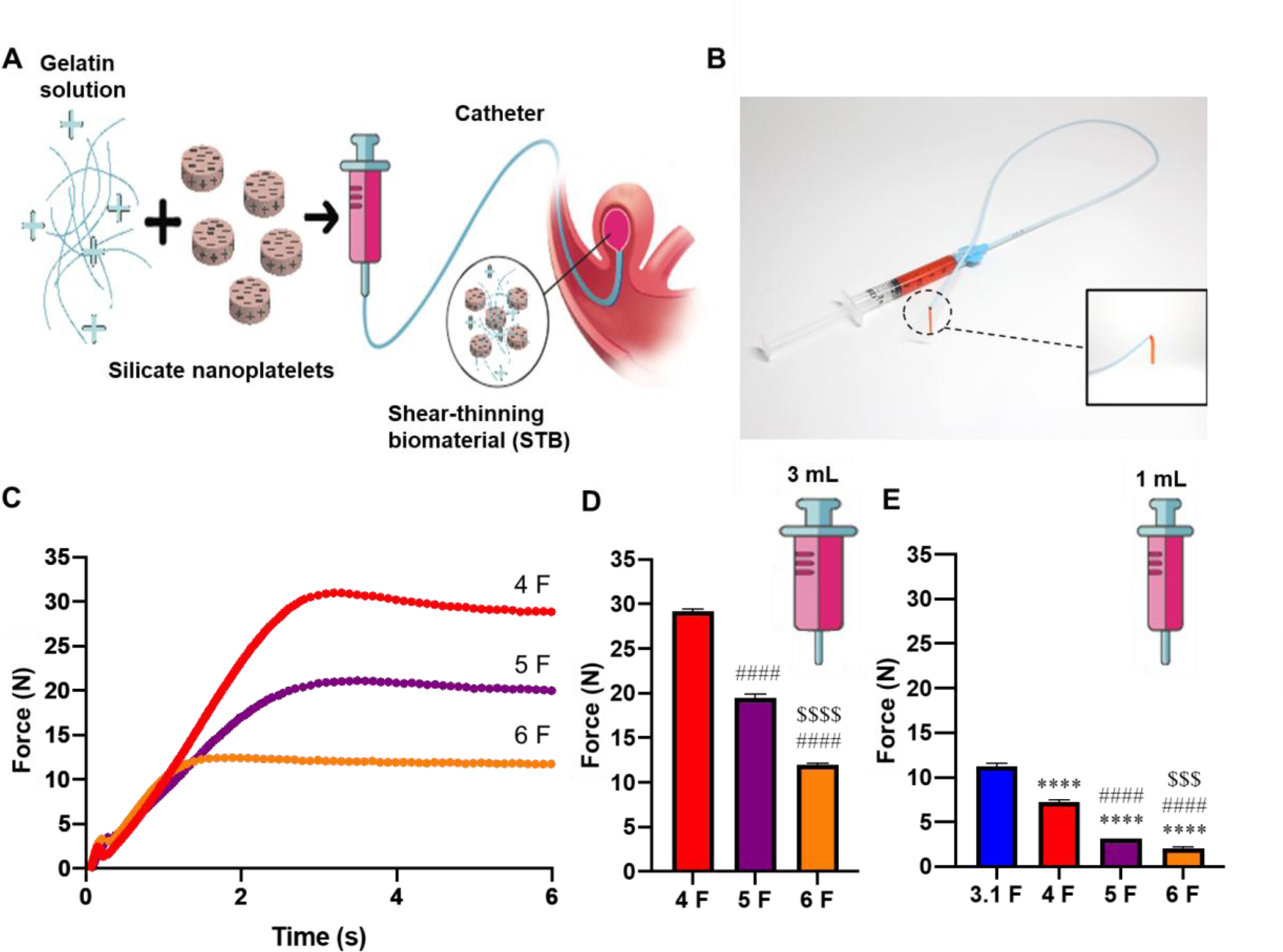
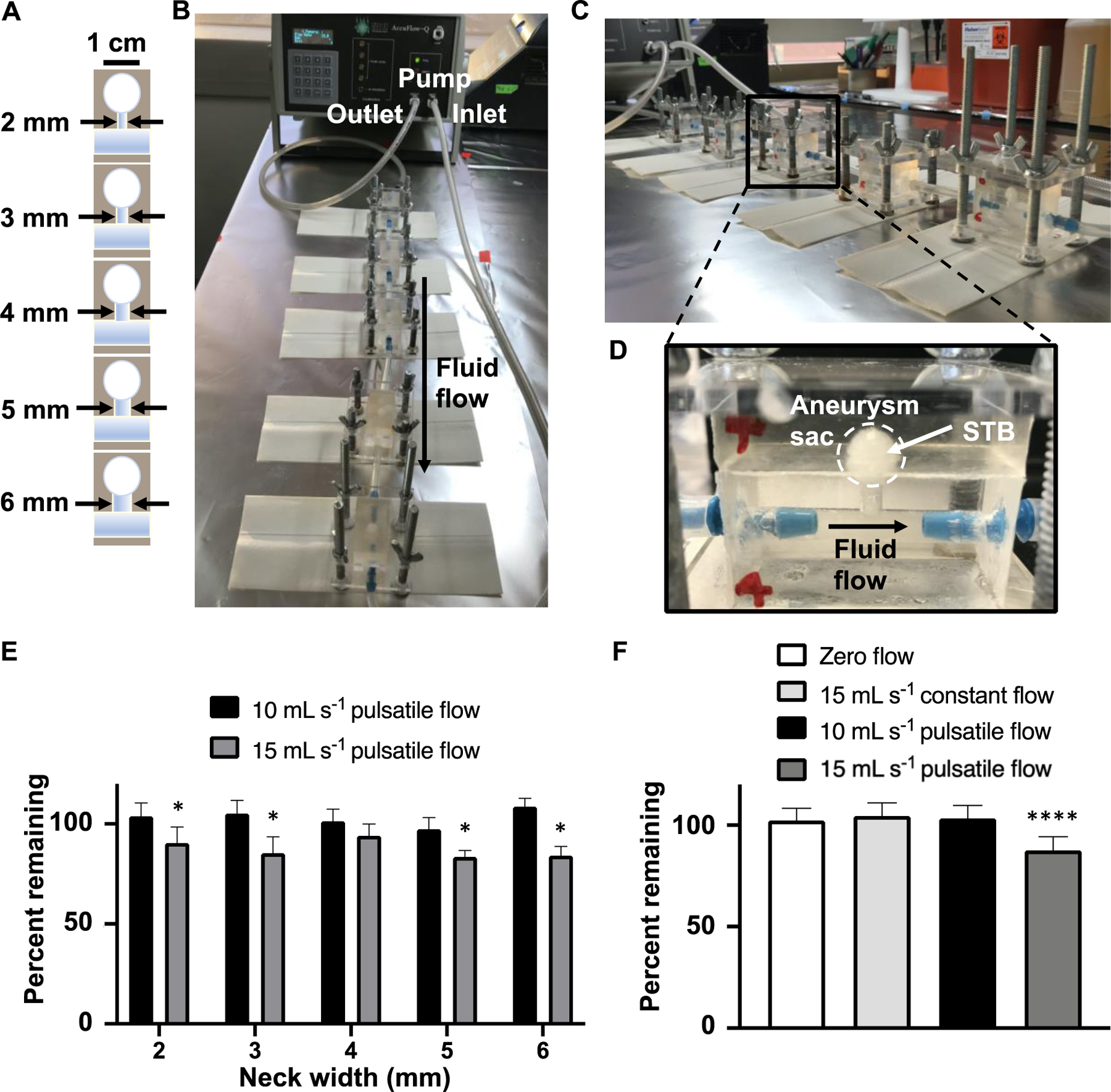
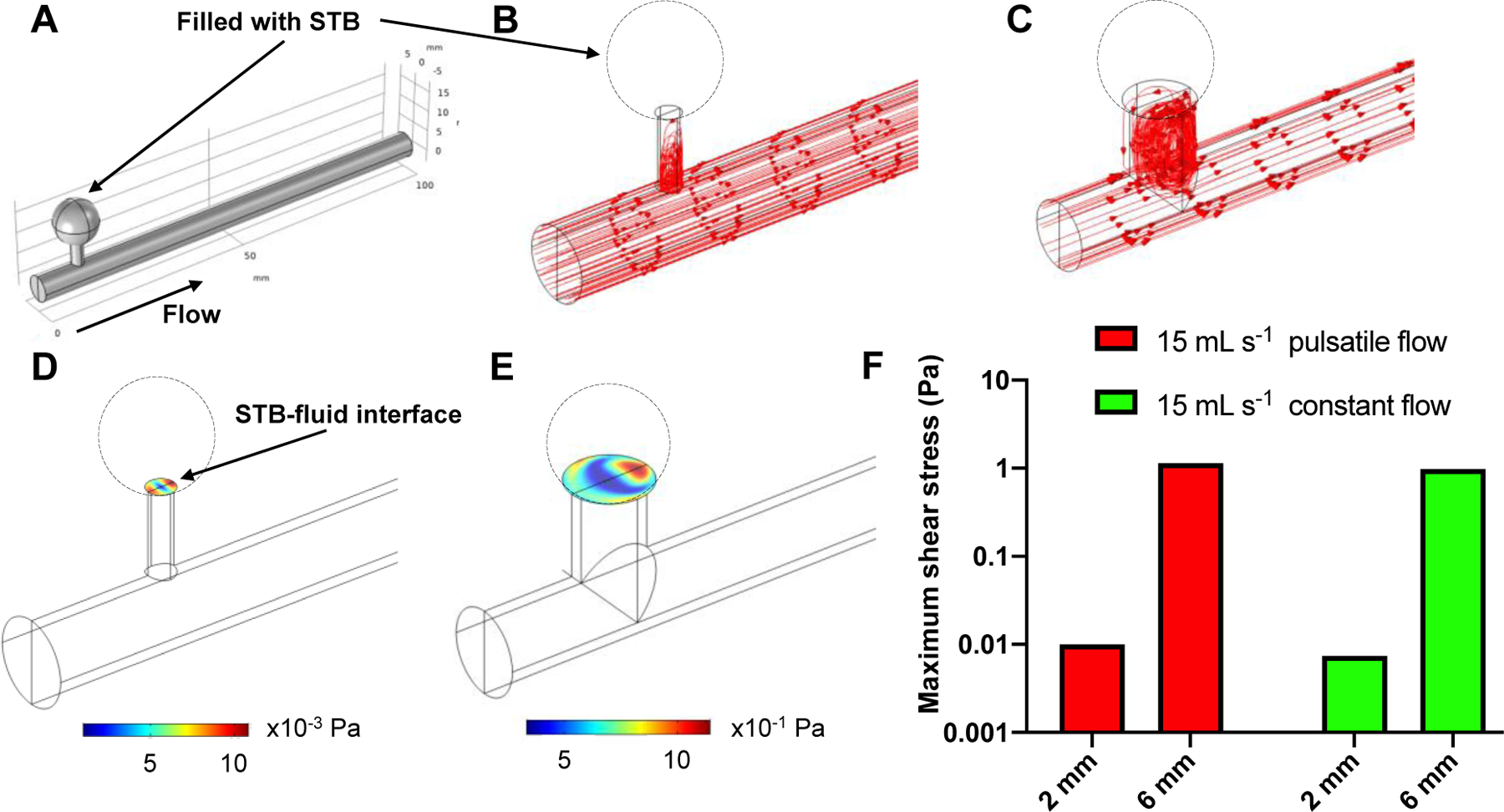
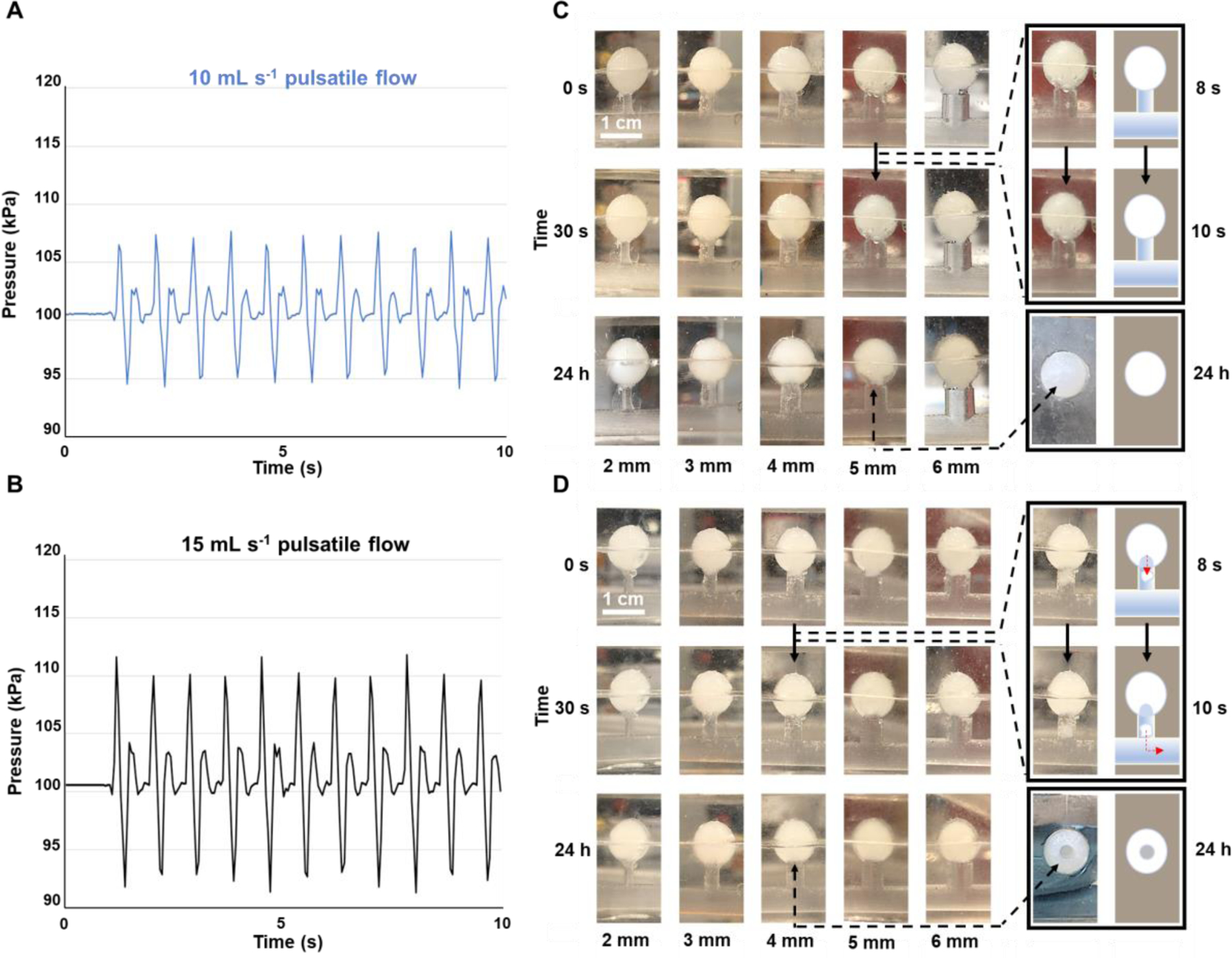
Metallic coil embolization is a common method for the endovascular treatment of visceral artery aneurysms (VAA) and visceral artery pseudoaneurysms (VAPA); however, this treatment is suboptimal due to the high cost of coils, incomplete volume occlusion, poor reendothelialization, aneurysm puncture, and coil migration. Several alternative treatment strategies are available, including stent flow diverters, glue embolics, gelfoam slurries, and vascular mesh plugs-each of which have their own disadvantages. Here, we investigated the in vitro capability of a shear-thinning biomaterial (STB), a nanocomposite hydrogel composed of gelatin and silicate nanoplatelets, for the minimally-invasive occlusion of simple necked aneurysm models. We demonstrated the injectability of STB through various clinical catheters, engineered an in vitro testing apparatus to independently manipulate aneurysm neck diameter, fluid flow rate, and flow waveform, and tested the stability of STB within the models under various conditions. Our experiments show that STB is able to withstand at least 1.89 Pa of wall shear stress, as estimated by computational fluid dynamics. STB is also able to withstand up to 10 mL s-1 pulsatile flow with a waveform mimicking blood flow in the human femoral artery and tolerate greater pressure changes than those in the human aorta. We ultimately found that our in vitro system was limited by supraphysiologic pressure changes caused by aneurysm models with low compliance.
Keywords: Catheters; Hydrogels; Minimally invasive; Pseudoaneurysms; Shear-thinning biomaterials; Silicate nanoplatelets; Visceral artery aneurysms.
Copyright © 2022 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Conflict of Interest
A. K. is a co-founder of a start‐up company, Obsidio, Inc., which is based on shear‐thinning embolic materials.
Declaration of interests
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Ali Khademhosseini reports financial support was provided by National Institutes of Health. Ali Khademhosseini reports a relationship with Obsidio, Inc that includes: board membership and equity or stocks. Ali Khademhosseini has patent Shear-thinning compositions as an intravascular embolic agent issued to Obsidio, Inc.
Figures