

Epidemiology of carbapenem-resistant and carbapenemase-producing Enterobacterales in the Netherlands 2017-2019
- PMID: 35397546
- PMCID: PMC8994189
- DOI: 10.1186/s13756-022-01097-9
Epidemiology of carbapenem-resistant and carbapenemase-producing Enterobacterales in the Netherlands 2017-2019
Abstract
Background: The Netherlands is currently considered a low endemic country for carbapenem-resistant Enterobacterales (CRE) and carbapenemase-producing Enterobacterales (CPE), experiencing only sporadic hospital outbreaks. This study aims to describe susceptibility to carbapenems and the epidemiology of carbapenemase production in Enterobacterales in the Netherlands in 2017-2019.
Methods: Three complementary nationwide surveillance systems are in place to monitor carbapenem susceptibility in the Netherlands. Routine antimicrobial susceptibility test results from medical microbiology laboratories were used to study phenotypic susceptibility of Escherichia coli and Klebsiella pneumoniae. Pathogen surveillance (of all Enterobacterales species) and mandatory notifications were used to describe the characteristics of CPE positive isolates and affected persons.
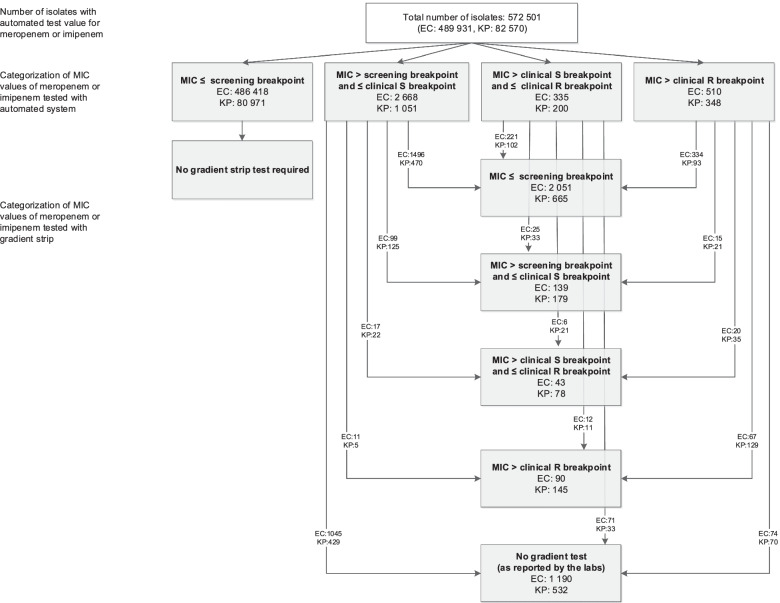
Results: The prevalence of isolates with gradient strip test-confirmed elevated meropenem (> 0.25 mg/L) or imipenem (> 1 mg/L) minimum inhibitory concentration (MIC) in the Netherlands was very low in 2017-2019, with percentages of 0.06% in E. coli and 0.49% in K. pneumoniae, and carbapenem resistances of 0.02% and 0.18%, respectively. A total of 895 unique species/carbapenemase-encoding allele combinations of CPE from 764 persons were submitted between 2017 and 2019, with the annual number of submissions increasing slightly each year. Epidemiological data was available for 660 persons. Screening because of presumed colonisation risk was the reason for sampling in 70.0% (462/660) of persons. Hospitalization abroad was the most common risk factor, being identified in 45.9% of persons.
Conclusions: Carbapenem resistance of E. coli and K. pneumoniae remains low in the Netherlands. The annual number of CPE isolates slightly increased during the period 2017-2019. Recent hospitalization abroad is the main risk factor for acquisition of CPE.
Keywords: Carbapenem resistance; Carbapenemase production; E. coli; Enterobacterales; Hospitalization; K. pneumoniae; Risk factors; Surveillance; Travel.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Brolund A, Lagerqvist N, Byfors S, Struelens MJ, Monnet DL, Albiger B, et al. Worsening epidemiological situation of carbapenemase-producing Enterobacteriaceae in Europe, assessment by national experts from 37 countries, July 2018. Euro Surveill. 2019;24(9):66. doi: 10.2807/1560-7917.ES.2019.24.9.1900123. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
