

Clinical phenotyping in sarcoidosis using cluster analysis
- PMID: 35397561
- PMCID: PMC8994095
- DOI: 10.1186/s12931-022-01993-z
Clinical phenotyping in sarcoidosis using cluster analysis
Abstract
Background: Most phenotyping paradigms in sarcoidosis are based on expert opinion; however, no paradigm has been widely adopted because of the subjectivity in classification. We hypothesized that cluster analysis could be performed on common clinical variables to define more objective sarcoidosis phenotypes.
Methods: We performed a retrospective cohort study of 554 sarcoidosis cases to identify distinct phenotypes of sarcoidosis based on 29 clinical features. Model-based clustering was performed using the VarSelLCM R package and the Integrated Completed Likelihood (ICL) criteria were used to estimate number of clusters. To identify features associated with cluster membership, features were ranked based on variable importance scores from the VarSelLCM model, and additional univariate tests (Fisher's exact test and one-way ANOVA) were performed using q-values correcting for multiple testing. The Wasfi severity score was also compared between clusters.
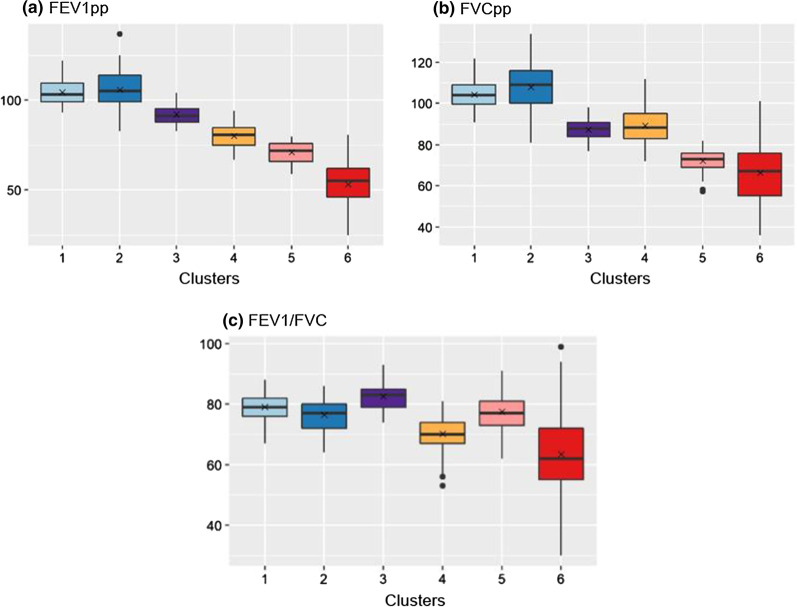
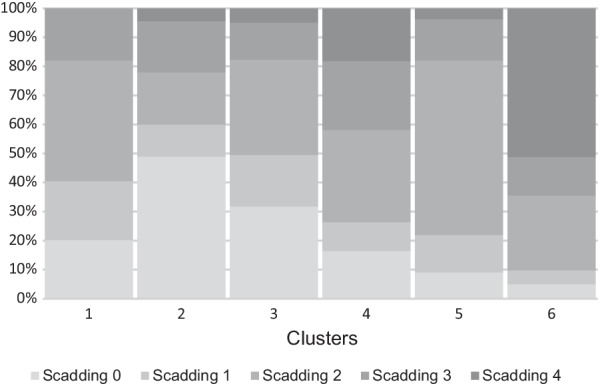
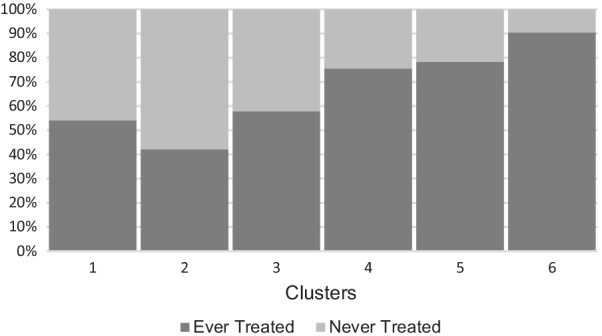
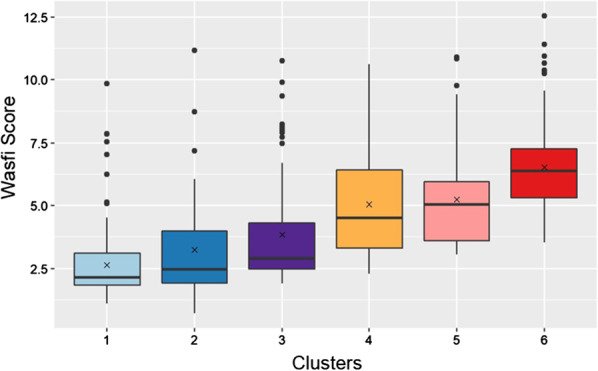
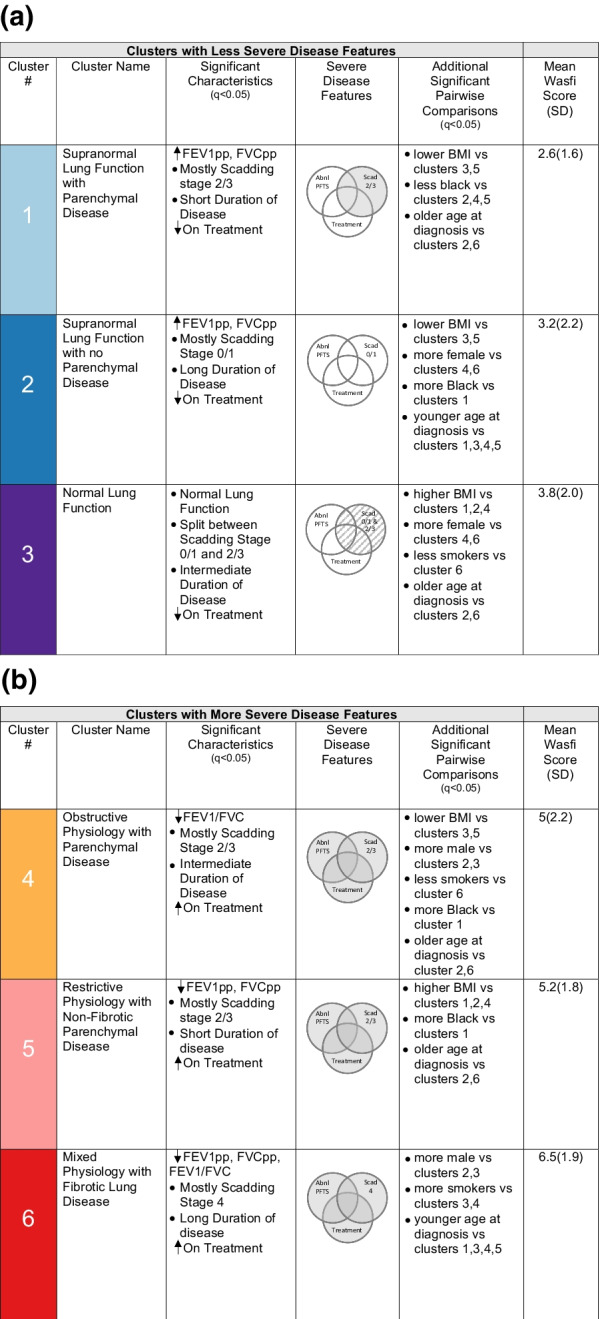
Results: Cluster analysis resulted in 6 sarcoidosis phenotypes. Salient characteristics for each cluster are as follows: Phenotype (1) supranormal lung function and majority Scadding stage 2/3; phenotype (2) supranormal lung function and majority Scadding stage 0/1; phenotype (3) normal lung function and split Scadding stages between 0/1 and 2/3; phenotype (4) obstructive lung function and majority Scadding stage 2/3; phenotype (5) restrictive lung function and majority Scadding stage 2/3; phenotype (6) mixed obstructive and restrictive lung function and mostly Scadding stage 4. Although there were differences in the percentages, all Scadding stages were encompassed by all of the phenotypes, except for phenotype 1, in which none were Scadding stage 4. Clusters 4, 5, 6 were significantly more likely to have ever been on immunosuppressive treatment and had higher Wasfi disease severity scores.
Conclusions: Cluster analysis produced 6 sarcoidosis phenotypes that demonstrated less severe and severe phenotypes. Phenotypes 1, 2, 3 have less lung function abnormalities, a lower percentage on immunosuppressive treatment and lower Wasfi severity scores. Phenotypes 4, 5, 6 were characterized by lung function abnormalities, more parenchymal abnormalities, an increased percentage on immunosuppressive treatment and higher Wasfi severity scores. These data support using cluster analysis as an objective and clinically useful way to phenotype sarcoidosis subjects and to empower clinicians to identify those with more severe disease versus those who have less severe disease, independent of Scadding stage.
Keywords: Cluster analysis; Disease severity; Phenotypes; Pulmonary; Sarcoidosis.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Statement on sarcoidosis. Joint Statement of the American Thoracic Society (ATS), the European Respiratory Society (ERS) and the World Association of Sarcoidosis and Other Granulomatous Disorders (WASOG) adopted by the ATS Board of Directors and by the ER. Am J Respir Crit Care Med. 1999;160(2):736-755. 10.1164/ajrccm.160.2.ats4-99. - PubMed
-
- Viskum K, Vestbo J. Vital prognosis in intrathoracic sarcoidosis with special reference to pulmonary function and radiological stage. Eur Respir J. 1993;6(3):349–353. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
