

Cup positioning and its effect on polyethylene wear of vitamin E- and non-vitamin E-supplemented liners in total hip arthroplasty: radiographic outcome at 5-year follow-up
- PMID: 35397656
- PMCID: PMC9957849
- DOI: 10.1007/s00402-022-04424-2
Cup positioning and its effect on polyethylene wear of vitamin E- and non-vitamin E-supplemented liners in total hip arthroplasty: radiographic outcome at 5-year follow-up
Abstract
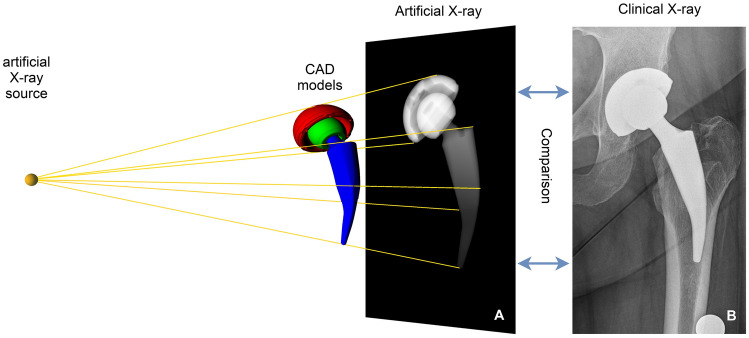
Background: Aseptic loosening remains a challenging problem after total hip arthroplasty. Accurate cup placement and supplementation of antioxidants in acetabular liners might reduce material failure rates. The aim of this study is to assess the effect of the cup position on the wear behaviour of UHMWPE-XE and UHMWPE-X liners in vivo using virtual radiographs.
Methods: We conducted a prospective, randomized, controlled, multicenter trial. Clinical data of 372 probands were analyzed. Anteroposterior pelvic X-rays of 324 patients immediately postoperatively and after 1 and 5 years were evaluated by the RayMatch® analysis software regarding cup position and wear behaviour.
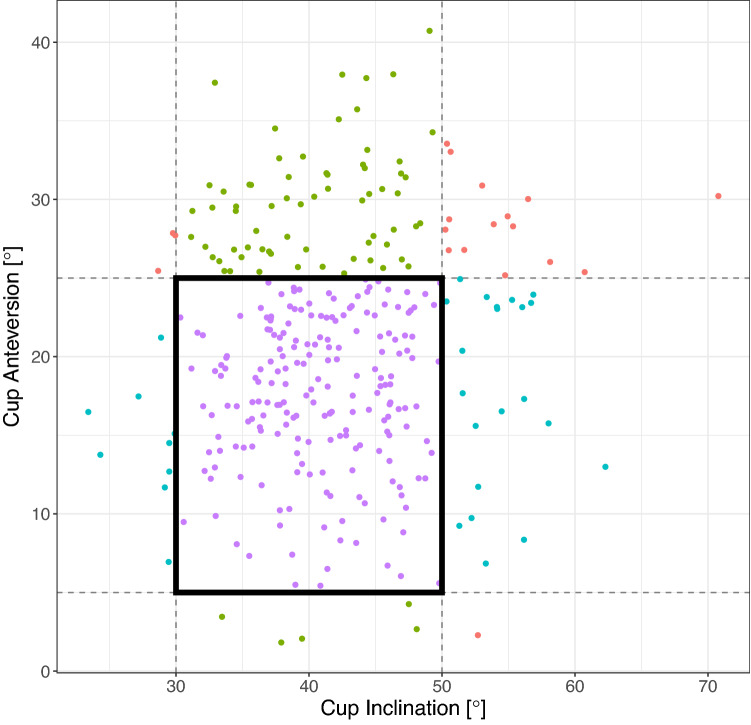
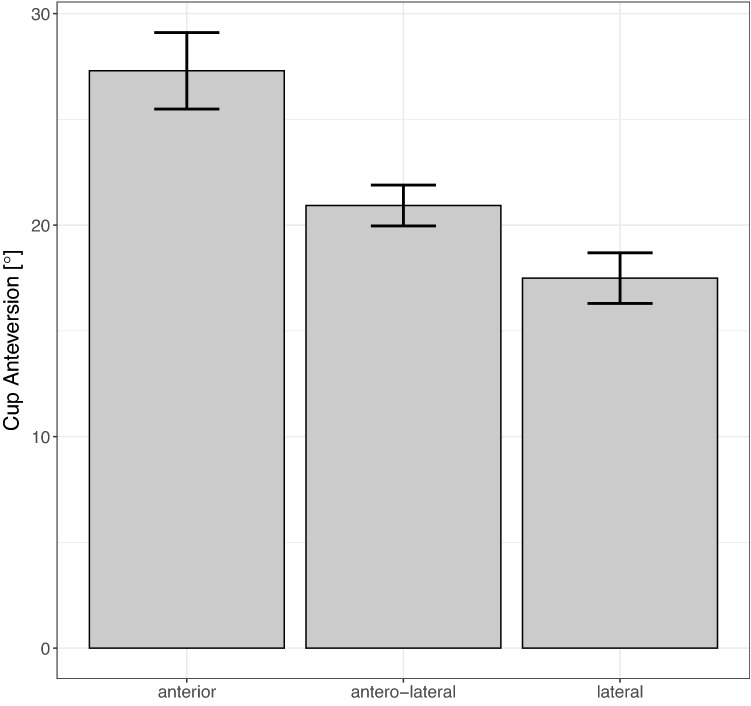
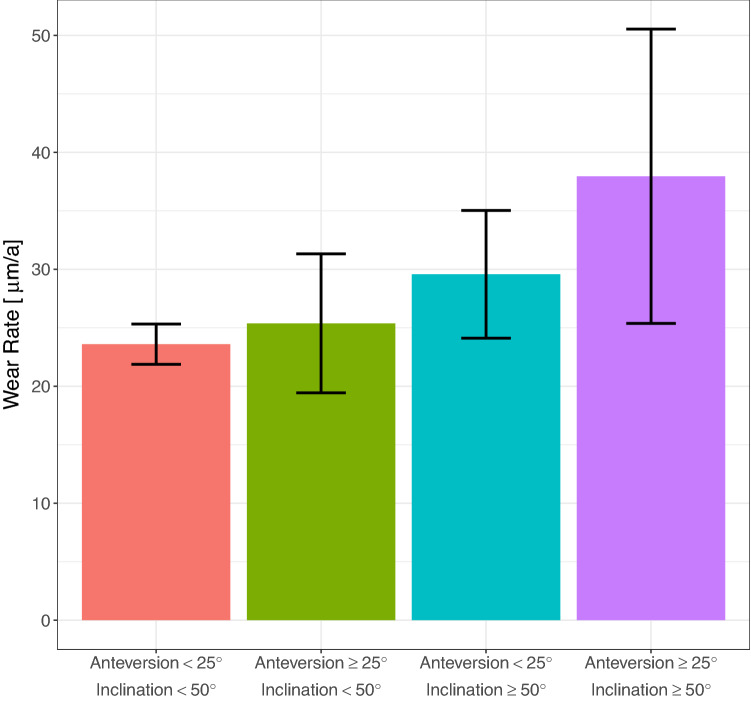
Results: Mean cup anteversion was 20.3° (± 7.4) and inclination was 41.9° (± 7.0) postoperatively. 62.3% of all patients had an anteversion and inclination within the Lewinnek safe zone. Anterior and anterolateral approaches led to significantly higher cup anteversion compared to lateral approaches (27.3° ± 5.5; 20.9° ± 7.2; 17.5° ± 6.6; p < 0.001 and p = 0.001, respectively). Mean anteversion increased to 24.6° (± 8.0) after 1 year (p < 0.001). Only one revision occurred because of implant dislocation. Wear rates from UHMWPE-X and UHMWPE-XE did not differ significantly. Anteversion angles ≥ 25° correlated to increased polyethylene wear (23.7 µm/year ± 12.8 vs. 31.1 µm/year ± 22.8, p = 0.012) and this was amplified when inclination angles were ≥ 50° (23.6 µm/year ± 12.8 vs. 38.0 µm/year ± 22.7, p = 0.062).
Conclusion: Anterior approaches lead to the highest inaccuracy of cup placement, but cup positioning outside the Lewinnek safe zone does not necessarily cause higher dislocation rates. Moreover, mean anteversion increased by approximately four degrees within the first year after operation, which is expected to be functional due to a regularization of pelvic tilt after intervention. Mid-term wear rates of UHMWPE-X and UHMWPE-XE liners are comparable, but steep cup positions lead to significantly increased polyethylene wear. In summary, a re-evaluation of target zones for intraoperative cup positioning might be considered. In the long-term reduced oxidative embrittlement could lead to superior wear behaviour of vitamin E-blended liners.
Keywords: CAD-based wear analysis; Cup placement; Total hip arthroplasty; UHMWPE-XE.
© 2022. The Author(s).
Conflict of interest statement
Alexander Roth is an employee of Aesculap AG, Tuttlingen. Otherwise the authors declare that they have no competing interests to declare that are relevant to the content of this article.
Figures
Similar articles
-
Vitamin E-blended highly cross-linked polyethylene liners in total hip arthroplasty: a randomized, multicenter trial using virtual CAD-based wear analysis at 5-year follow-up.Arch Orthop Trauma Surg. 2020 Dec;140(12):1859-1866. doi: 10.1007/s00402-020-03358-x. Epub 2020 Feb 12. Arch Orthop Trauma Surg. 2020. PMID: 32048017 Clinical Trial.
-
The Safe Zone Range for Cup Anteversion Is Narrower Than for Inclination in THA.Clin Orthop Relat Res. 2018 Feb;476(2):325-335. doi: 10.1007/s11999.0000000000000051. Clin Orthop Relat Res. 2018. PMID: 29529664 Free PMC article.
-
A vitamin E blended highly cross-linked polyethylene acetabular cup results in less wear: 6-year results of a randomized controlled trial in 199 patients.Acta Orthop. 2020 Dec;91(6):705-710. doi: 10.1080/17453674.2020.1807220. Epub 2020 Aug 24. Acta Orthop. 2020. PMID: 32835560 Free PMC article. Clinical Trial.
-
Does intraoperative fluoroscopy improve acetabular component positioning and limb-length discrepancy during direct anterior total hip arthroplasty? A meta-analysis.J Orthop Surg Res. 2023 Aug 8;18(1):586. doi: 10.1186/s13018-023-04023-w. J Orthop Surg Res. 2023. PMID: 37553600 Free PMC article.
-
In Vivo Performance of Vitamin E Stabilized Polyethylene Implants for Total Hip Arthroplasty: A Review.J Arthroplasty. 2023 May;38(5):970-979. doi: 10.1016/j.arth.2022.11.010. Epub 2022 Dec 5. J Arthroplasty. 2023. PMID: 36481286 Review.
Cited by
-
Polyethylene liner dissociation in total hip arthroplasty: a retrospective case-control study on a single implant design.J Orthop Traumatol. 2024 Aug 14;25(1):38. doi: 10.1186/s10195-024-00785-z. J Orthop Traumatol. 2024. PMID: 39143399 Free PMC article.
-
The addition of vitamin E could reduce femoral head penetration of the polyethylene liners.J Orthop Surg Res. 2025 Jan 20;20(1):72. doi: 10.1186/s13018-024-05402-7. J Orthop Surg Res. 2025. PMID: 39833940 Free PMC article.
-
Vitamin E-enriched medium cross-linked polyethylene in total knee arthroplasty (VIKEP): clinical outcome, oxidation profile, and wear analysis in comparison to standard polyethylene-study protocol for a randomized controlled trial.Trials. 2024 Jan 5;25(1):27. doi: 10.1186/s13063-023-07811-1. Trials. 2024. PMID: 38183062 Free PMC article.
-
Metal-on-crosslinked polyethylene in total hip arthroplasty - an excellent combination at fifteen to twenty years of follow-up.Int Orthop. 2023 Oct;47(10):2547-2552. doi: 10.1007/s00264-023-05844-4. Epub 2023 May 29. Int Orthop. 2023. PMID: 37247019
-
Updates on Biomaterials Used in Total Hip Arthroplasty (THA).Polymers (Basel). 2023 Aug 2;15(15):3278. doi: 10.3390/polym15153278. Polymers (Basel). 2023. PMID: 37571172 Free PMC article. Review.
References
-
- Hailer NP, Weiss RJ, Stark A, Karrholm J. The risk of revision due to dislocation after total hip arthroplasty depends on surgical approach, femoral head size, sex, and primary diagnosis. an analysis of 78,098 operations in the Swedish Hip Arthroplasty Register. Acta Orthop. 2012;83:442–448. doi: 10.3109/17453674.2012.733919. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
