

The age-dependent association of risk factors with pancreatic cancer
- PMID: 35398288
- PMCID: PMC9233063
- DOI: 10.1016/j.annonc.2022.03.276
The age-dependent association of risk factors with pancreatic cancer
Abstract
Background: Pancreatic cancer presents as advanced disease in >80% of patients; yet, appropriate ages to consider prevention and early detection strategies are poorly defined. We investigated age-specific associations and attributable risks of pancreatic cancer for established modifiable and non-modifiable risk factors.
Patients and methods: We included 167 483 participants from two prospective US cohort studies with 1190 incident cases of pancreatic cancer during >30 years of follow-up; 5107 pancreatic cancer cases and 8845 control participants of European ancestry from a completed multicenter genome-wide association study (GWAS); and 248 893 pancreatic cancer cases documented in the US Surveillance, Epidemiology, and End Results (SEER) Program. Across different age categories, we investigated cigarette smoking, obesity, diabetes, height, and non-O blood group in the prospective cohorts; weighted polygenic risk score of 22 previously identified single nucleotide polymorphisms in the GWAS; and male sex and black race in the SEER Program.
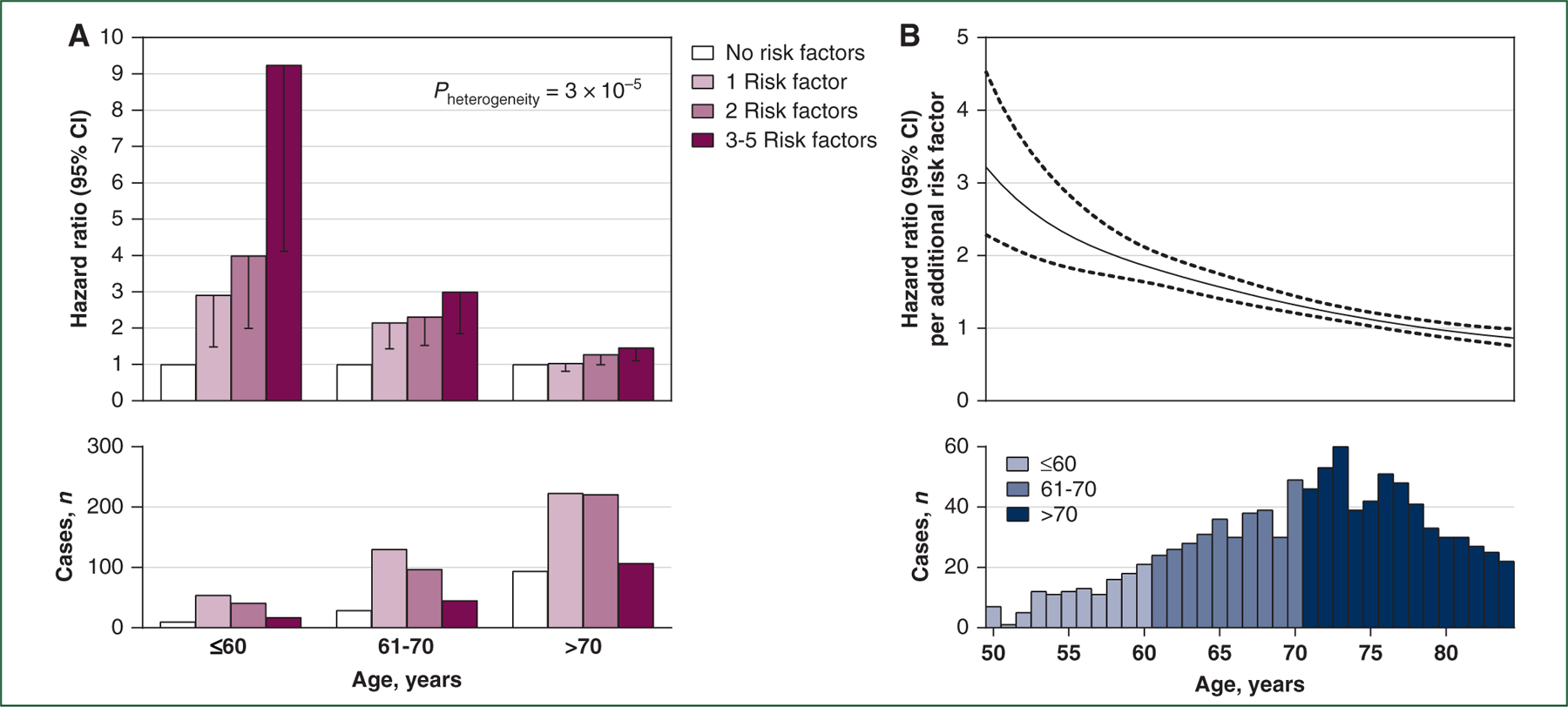
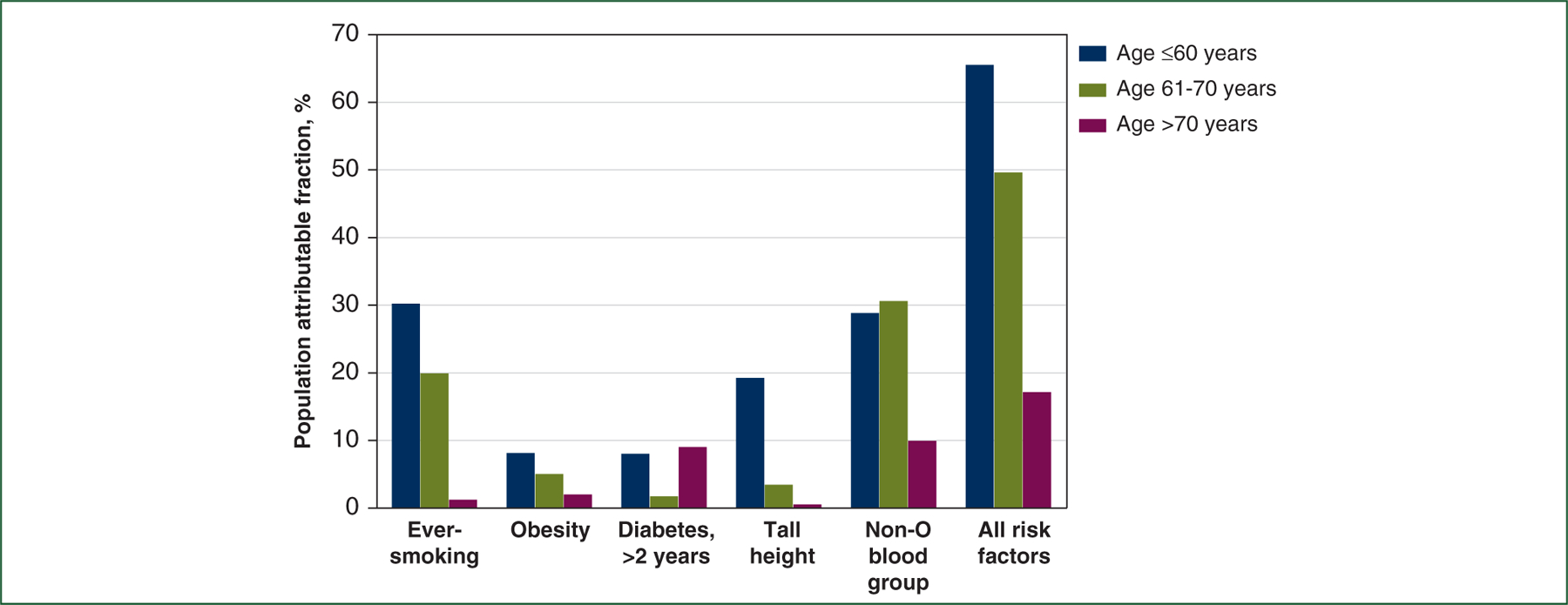
Results: In the prospective cohorts, all five risk factors were more strongly associated with pancreatic cancer risk among younger participants, with associations attenuated among those aged >70 years. The hazard ratios comparing participants with three to five risk factors with those with no risk factors were 9.24 [95% confidence interval (CI) 4.11-20.77] among those aged ≤60 years, 3.00 (95% CI 1.85-4.86) among those aged 61-70 years, and 1.46 (95% CI 1.10-1.94) among those aged >70 years (Pheterogeneity = 3×10-5). These factors together were related to 65.6%, 49.7%, and 17.2% of incident pancreatic cancers in these age groups, respectively. In the GWAS and the SEER Program, the associations with the polygenic risk score, male sex, and black race were all stronger among younger individuals (Pheterogeneity ≤0.01).
Conclusions: Established risk factors are more strongly associated with earlier-onset pancreatic cancer, emphasizing the importance of age at initiation for cancer prevention and control programs targeting this highly lethal malignancy.
Keywords: age; lifestyle modification; pancreatic cancer; polygenic risk score; risk factor.
Copyright © 2022 European Society for Medical Oncology. All rights reserved.
Figures
References
-
- Siegel RL, Miller KD, Fuchs HE, Jemal A. Cancer statistics, 2021. CA Cancer J Clin 2021;71:7–33. - PubMed
-
- Howlader N, Noone AM, Krapcho M, et al. SEER Cancer Statistics Review, 1975–2017 Bethesda, MD: National Cancer Institute; 2020. Available at https://seer.cancer.gov/csr/1975_2017/. Accessed December 1, 2020.
-
- Tavakkoli A, Singal AG, Waljee AK, et al. Racial disparities and trends in pancreatic cancer incidence and mortality in the United States. Clin Gastroenterol Hepatol 2020;18:171–178 e110. - PubMed
-
- Sung H, Siegel RL, Rosenberg PS, Jemal A. Emerging cancer trends among young adults in the USA: analysis of a population-based cancer registry. Lancet Public Health 2019;4:e137–e147. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
