

Patient characteristics, management and outcomes in a Nordic subset of the "large observational study to understand the global impact of severe acute respiratory failure" (LUNG SAFE) study
- PMID: 35398892
- PMCID: PMC9322410
- DOI: 10.1111/aas.14069
Patient characteristics, management and outcomes in a Nordic subset of the "large observational study to understand the global impact of severe acute respiratory failure" (LUNG SAFE) study
Abstract
Background: The "Large observational study to understand the global impact of severe acute respiratory failure" (LUNG SAFE) study described the worldwide epidemiology and management of patients with acute hypoxaemic respiratory failure (AHRF). Here, we present the Nordic subset of data from the LUNG SAFE cohort.
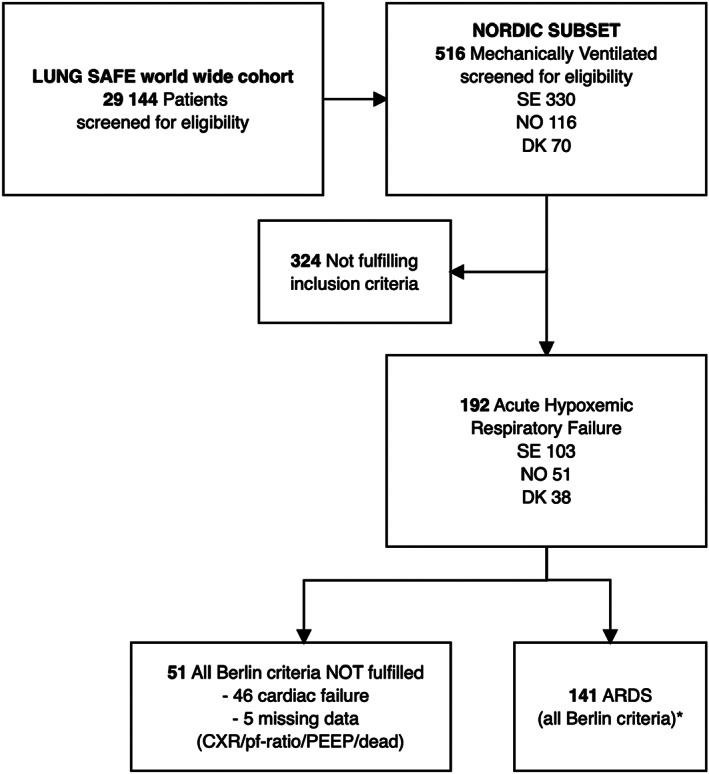
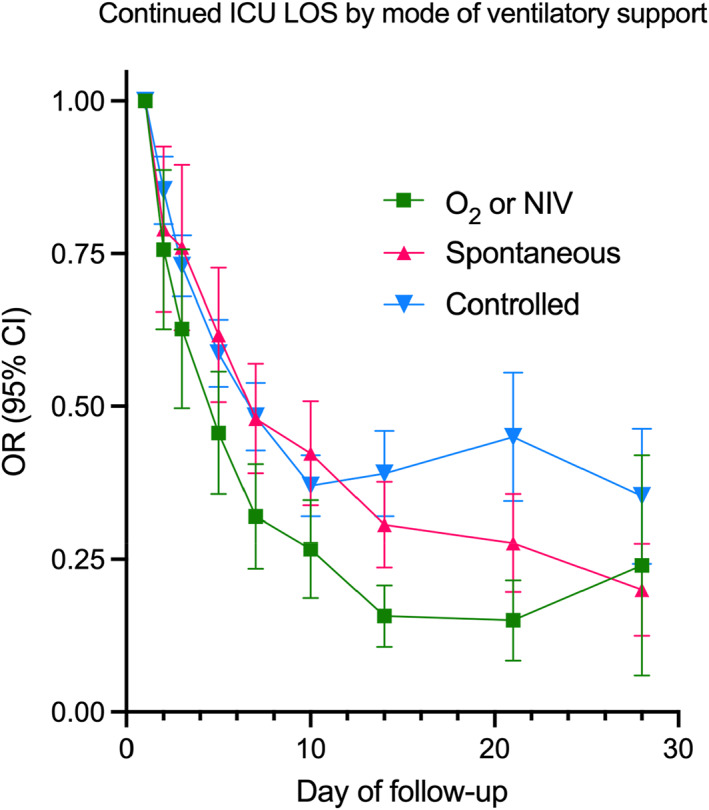
Methods: We extracted LUNG SAFE data for adults fulfilling criteria for AHRF in intensive care units (ICU) in Denmark, Norway and Sweden, including demographics, co-morbidities, clinical assessment and management characteristics, 90-day survival and length-of-stay (LOS). We analysed ICU LOS with linear regression, and associations between risk factors and mortality were quantified using Cox regression.
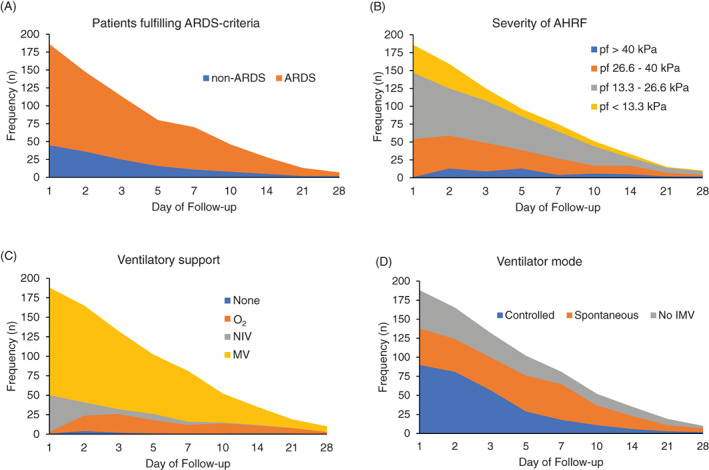
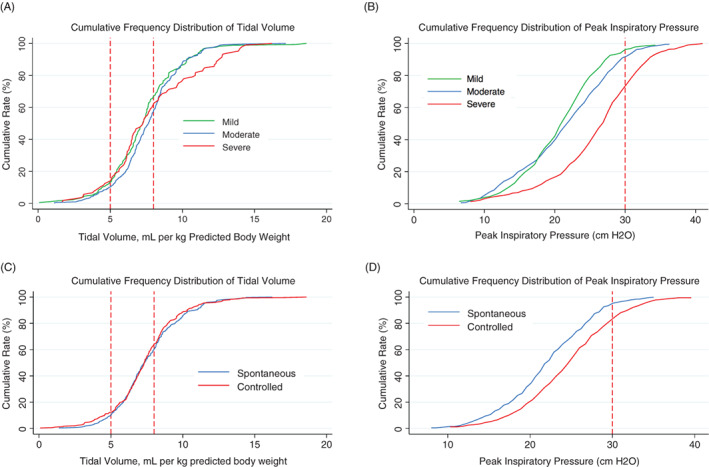
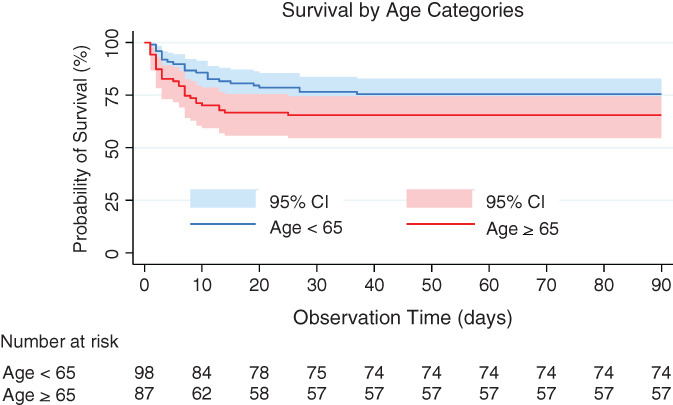
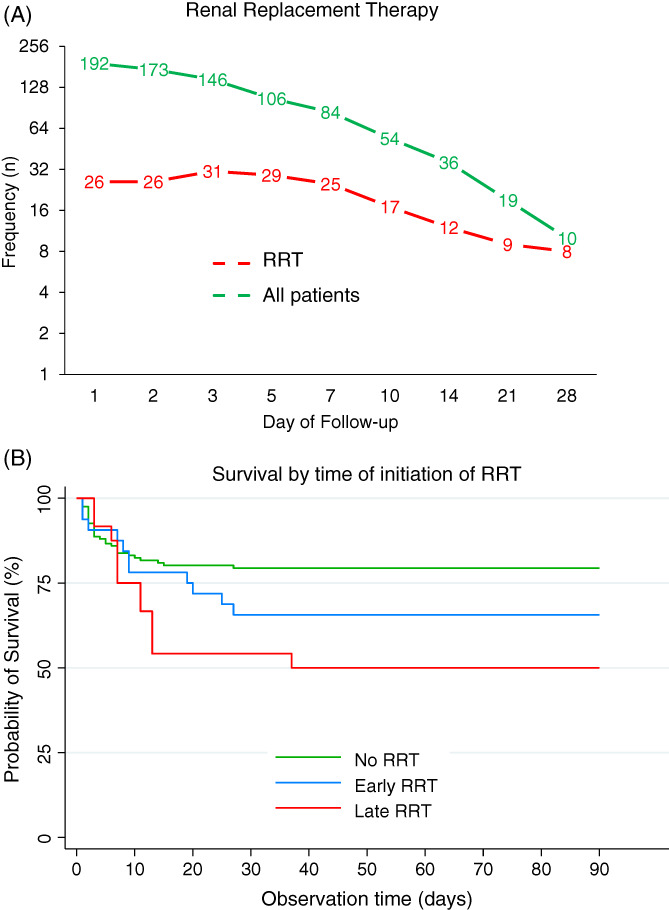
Results: We included 192 patients, with a median age of 64 years (IQR 55, 72), and a male-to-female ratio of 2:1. The majority had one or more co-morbidities, and clinicians identified pneumonia as the primary cause of respiratory failure in 56% and acute respiratory distress syndrome (ARDS) in 21%. Median ICU LOS and duration of invasive mechanical ventilation (IMV) were 5 and 3 days. Tidal volumes (TV) were frequently larger than that supported by evidence and IMV allowing for spontaneous ventilation was common. Younger age, co-morbidity, surgical admission and ARDS were associated with ICU LOS. Sixty-one patients (32%) were dead at 90 days. Age and a non-surgical cause of admission were associated with death.
Conclusions: In this subset of LUNG SAFE, ARDS was often not recognised in patients with AHRF and management frequently deviated from evidence-based practices. ICU LOS was generally short, and mortality was attributable to known risk factors.
© 2022 The Authors. Acta Anaesthesiologica Scandinavica published by John Wiley & Sons Ltd on behalf of Acta Anaesthesiologica Scandinavica Foundation.
Figures
Similar articles
-
Identifying associations between diabetes and acute respiratory distress syndrome in patients with acute hypoxemic respiratory failure: an analysis of the LUNG SAFE database.Crit Care. 2018 Oct 27;22(1):268. doi: 10.1186/s13054-018-2158-y. Crit Care. 2018. PMID: 30367670 Free PMC article.
-
Epidemiology, Patterns of Care, and Mortality for Patients With Acute Respiratory Distress Syndrome in Intensive Care Units in 50 Countries.JAMA. 2016 Feb 23;315(8):788-800. doi: 10.1001/jama.2016.0291. JAMA. 2016. PMID: 26903337
-
Acute respiratory failure requiring mechanical ventilation in severe chronic obstructive pulmonary disease (COPD).Medicine (Baltimore). 2018 Apr;97(17):e0487. doi: 10.1097/MD.0000000000010487. Medicine (Baltimore). 2018. PMID: 29703009 Free PMC article.
-
Effectiveness of dexmedetomidine versus propofol on extubation times, length of stay and mortality rates in adult cardiac surgery patients: a systematic review and meta-analysis.JBI Database System Rev Implement Rep. 2018 May;16(5):1220-1239. doi: 10.11124/JBISRIR-2017-003488. JBI Database System Rev Implement Rep. 2018. PMID: 29762314
-
Evidence-Based Practices for Acute Respiratory Failure and Acute Respiratory Distress Syndrome: A Systematic Review of Reviews.Chest. 2020 Dec;158(6):2381-2393. doi: 10.1016/j.chest.2020.06.080. Epub 2020 Jul 16. Chest. 2020. PMID: 32682771 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
