

Variations in end-of-life care practices in older critically ill patients with COVID-19 in Europe
- PMID: 35398948
- PMCID: PMC9115222
- DOI: 10.1111/joim.13492
Variations in end-of-life care practices in older critically ill patients with COVID-19 in Europe
Abstract
Background: Previous studies reported regional differences in end-of-life care (EoLC) for critically ill patients in Europe.
Objectives: The purpose of this post-hoc analysis of the prospective multicentre COVIP study was to investigate variations in EoLC practices among older patients in intensive care units during the coronavirus disease 2019 pandemic.
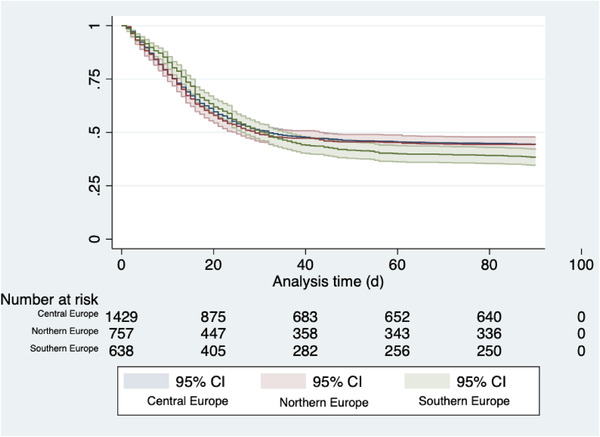
Methods: A total of 3105 critically ill patients aged 70 years and older were enrolled in this study (Central Europe: n = 1573; Northern Europe: n = 821; Southern Europe: n = 711). Generalised estimation equations were used to calculate adjusted odds ratios (aORs) to population averages. Data were adjusted for patient-specific variables (demographic, disease-specific) and health economic data (gross domestic product, health expenditure per capita). The primary outcome was any treatment limitation, and 90-day mortality was a secondary outcome.
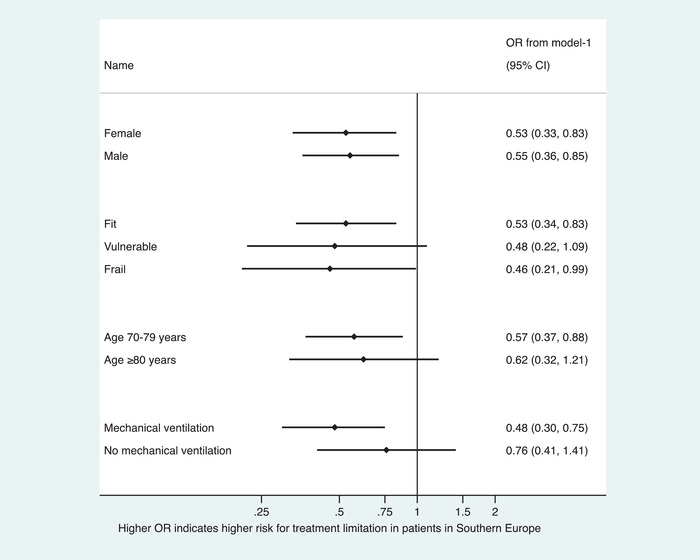
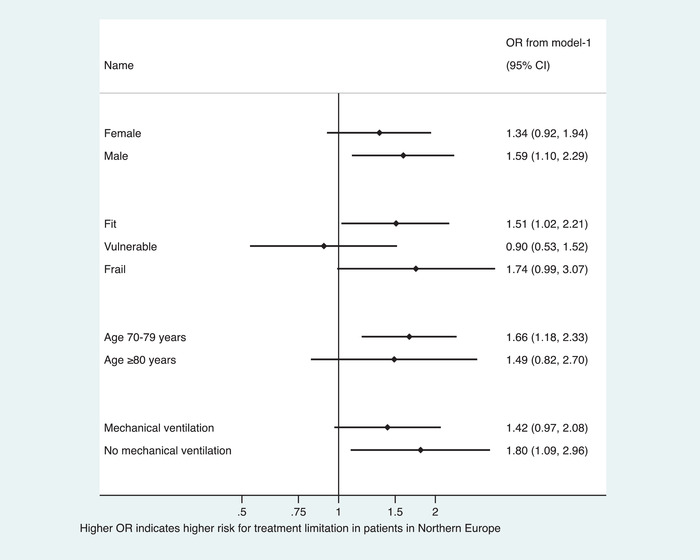
Results: The frequency of the primary endpoint (treatment limitation) was highest in Northern Europe (48%), intermediate in Central Europe (39%) and lowest in Southern Europe (24%). The likelihood for treatment limitations was lower in Southern than in Central Europe (aOR 0.39; 95% confidence interval [CI] 0.21-0.73; p = 0.004), even after multivariable adjustment, whereas no statistically significant differences were observed between Northern and Central Europe (aOR 0.57; 95%CI 0.27-1.22; p = 0.15). After multivariable adjustment, no statistically relevant mortality differences were found between Northern and Central Europe (aOR 1.29; 95%CI 0.80-2.09; p = 0.30) or between Southern and Central Europe (aOR 1.07; 95%CI 0.66-1.73; p = 0.78).
Conclusion: This study shows a north-to-south gradient in rates of treatment limitation in Europe, highlighting the heterogeneity of EoLC practices across countries. However, mortality rates were not affected by these results.
Keywords: COVID-19; critical care; frail elderly; public health systems research; resuscitation orders.
© 2022 The Authors. Journal of Internal Medicine published by John Wiley & Sons Ltd on behalf of Association for Publication of The Journal of Internal Medicine.
Conflict of interest statement
J.C.S. (full departmental disclosure) reports grants from Orion Pharma, Abbott Nutrition International, B. Braun Medical AG, CSEM AG, Edwards Lifesciences Services GmbH, Kenta Biotech Ltd, Maquet Critical Care AB, Omnicare Clinical Research AG, Nestle, Pierre Fabre Pharma AG, Pfizer, Bard Medica S.A., Abbott AG, Anandic Medical Systems, Pan Gas AG Healthcare, Bracco, Hamilton Medical AG, Fresenius Kabi, Getinge Group Maquet AG, Dräger AG, Teleflex Medical GmbH, Glaxo Smith Kline, Merck Sharp and Dohme AG, Eli Lilly and Company, Baxter, Astellas, Astra Zeneca, CSL Behring, Novartis, Covidien, Phagenesis and Nycomed outside of the submitted work. The money was paid into departmental funds. No personal financial gain applied. The other authors declare that they have no conflict of interests.
Figures
References
-
- Avidan A, Sprung CL, Schefold JC, Ricou B, Hartog CS, Nates JL, et al. Variations in end‐of‐life practices in intensive care units worldwide (Ethicus‐2): a prospective observational study. Lancet Respir Medicine. 2021;9(10):1101–10. - PubMed
-
- Guidet B, Flaatten H, Boumendil A, Morandi A, Andersen FH, Artigas A, et al. Withholding or withdrawing of life‐sustaining therapy in older adults (≥80 years) admitted to the intensive care unit. Intens Care Med. 2018;44(7):1027–38. - PubMed
-
- Flaatten H, De Lange DW, Jung C, Beil M, Guidet B. The impact of end‐of‐life care on ICU outcome. Intens Care Med. 2021;47:624–5. - PubMed
-
- Guidet B, De Lange DW, Flaatten H. Should this elderly patient be admitted to the ICU? Intens Care Med. 2018;44(11):1926–8. - PubMed
