

The effects of vitamin D supplementation on frailty in older adults at risk for falls
- PMID: 35399053
- PMCID: PMC8994906
- DOI: 10.1186/s12877-022-02888-w
The effects of vitamin D supplementation on frailty in older adults at risk for falls
Abstract
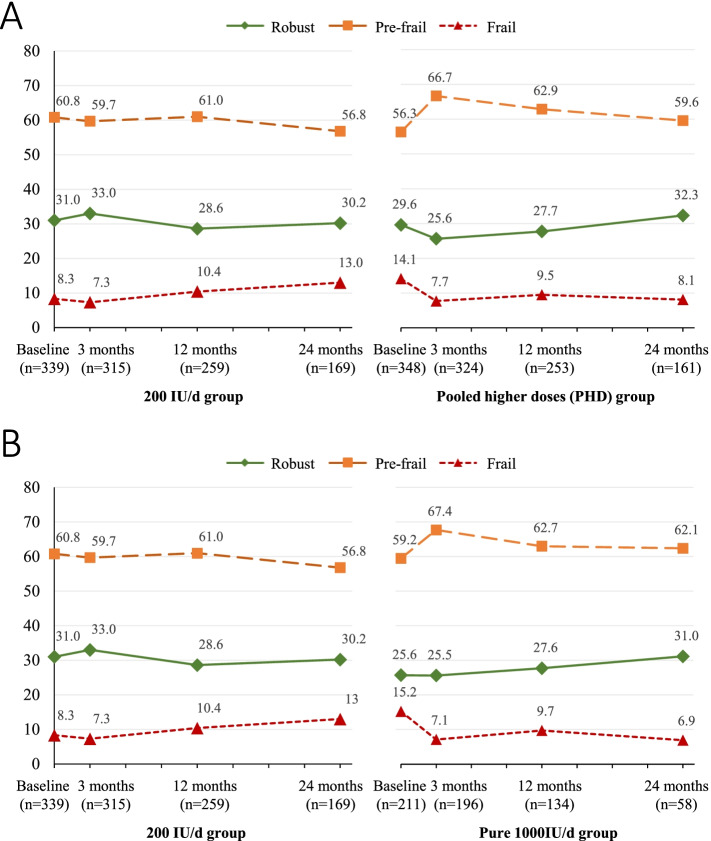
Background: Low serum 25-hydroxyvitamin D [25(OH)D] level is associated with a greater risk of frailty, but the effects of daily vitamin D supplementation on frailty are uncertain. This secondary analysis aimed to examine the effects of vitamin D supplementation on frailty using data from the Study To Understand Fall Reduction and Vitamin D in You (STURDY).
Methods: The STURDY trial, a two-stage Bayesian, response-adaptive, randomized controlled trial, enrolled 688 community-dwelling adults aged ≥ 70 years with a low serum 25(OH)D level (10-29 ng/mL) and elevated fall risk. Participants were initially randomized to 200 IU/d (control dose; n = 339) or a higher dose (1000 IU/d, 2000 IU/d, or 4000 IU/d; n = 349) of vitamin D3. Once the 1000 IU/d was selected as the best higher dose, other higher dose groups were reassigned to the 1000 IU/d group and new enrollees were randomized 1:1 to 1000 IU/d or control group. Data were collected at baseline, 3, 12, and 24 months. Frailty phenotype was based on number of the following conditions: unintentional weight loss, exhaustion, slowness, low activity, and weakness (≥ 3 conditions as frail, 1 or 2 as pre-frail, and 0 as robust). Cox proportional hazard models estimated the risk of developing frailty, or improving or worsening frailty status at follow-up. All models were adjusted for demographics, health conditions, and further stratified by baseline serum 25(OH)D level (insufficiency (20-29 ng/mL) vs. deficiency (10-19 ng/mL)).
Results: Among 687 participants (mean age 77.1 ± 5.4, 44% women) with frailty assessment at baseline, 208 (30%) were robust, 402 (59%) were pre-frail, and 77 (11%) were frail. Overall, there was no significant difference in risk of frailty outcomes comparing the pooled higher doses (PHD; ≥ 1000 IU/d) vs. 200 IU/d. When comparing each higher dose vs. 200 IU/d, the 2000 IU/d group had nearly double the risk of worsening frailty status (HR = 1.89, 95% CI: 1.13-3.16), while the 4000 IU/d group had a lower risk of developing frailty (HR = 0.22, 95% CI: 0.05-0.97). There were no significant associations between vitamin D doses and frailty status in the analyses stratified by baseline serum 25(OH)D level.
Conclusions: High dose vitamin D supplementation did not prevent frailty. Significant subgroup findings might be the results of type 1 error.
Trial registration: ClinicalTrials.gov: NCT02166333 .
Keywords: Frailty; Nutrition supplementation; Randomized controlled trial; Vitamin D3.
© 2022. The Author(s).
Conflict of interest statement
The authors do not have completing interests to declare.
Figures

References
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
