

External validation of the 2020 ERC/ESICM prognostication strategy algorithm after cardiac arrest
- PMID: 35399085
- PMCID: PMC8996564
- DOI: 10.1186/s13054-022-03954-w
External validation of the 2020 ERC/ESICM prognostication strategy algorithm after cardiac arrest
Abstract
Purpose: To assess the performance of the post-cardiac arrest (CA) prognostication strategy algorithm recommended by the European Resuscitation Council (ERC) and the European Society of Intensive Care Medicine (ESICM) in 2020.
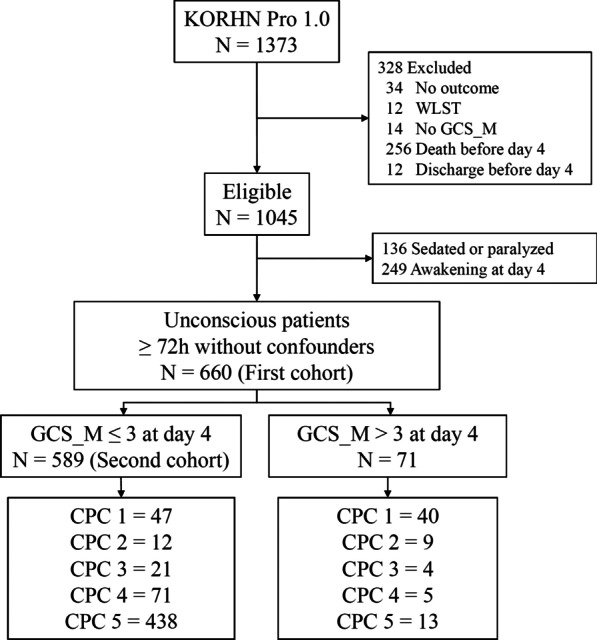
Methods: This was a retrospective analysis of the Korean Hypothermia Network Prospective Registry 1.0. Unconscious patients without confounders at day 4 (72-96 h) after return of spontaneous circulation (ROSC) were included. The association between the prognostic factors included in the prognostication strategy algorithm, except status myoclonus and the neurological outcome, was investigated, and finally, the prognostic performance of the prognostication strategy algorithm was evaluated. Poor outcome was defined as cerebral performance categories 3-5 at 6 months after ROSC.
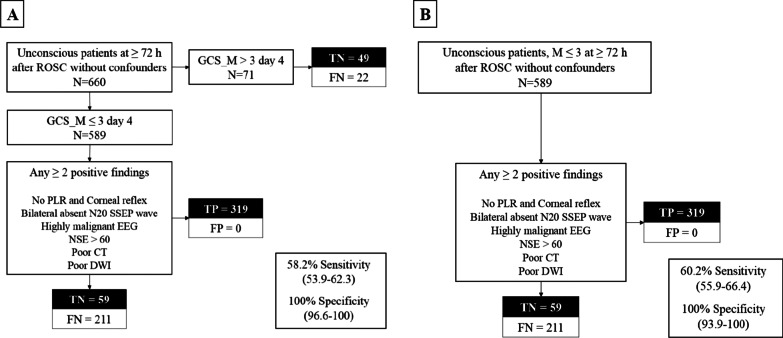
Results: A total of 660 patients were included in the final analysis. Of those, 108 (16.4%) patients had a good neurological outcome at 6 months after CA. The 2020 ERC/ESICM prognostication strategy algorithm identified patients with poor neurological outcome with 60.2% sensitivity (95% CI 55.9-64.4) and 100% specificity (95% CI 93.9-100) among patients who were unconscious or had a GCS_M score ≤ 3 and with 58.2% sensitivity (95% CI 53.9-62.3) and 100% specificity (95% CI 96.6-100) among unconscious patients. When two prognostic factors were combined, any combination of prognostic factors had a false positive rate (FPR) of 0 (95% CI 0-5.6 for combination of no PR/CR and poor CT, 0-30.8 for combination of No SSEP N20 and NSE 60).
Conclusion: The 2020 ERC/ESICM prognostication strategy algorithm predicted poor outcome without an FPR and with sensitivities of 58.2-60.2%. Any combinations of two predictors recommended by ERC/ESICM showed 0% of FPR.
Keywords: Cardiac arrest; Guideline algorithm; Outcome; Prognostic accuracy.
© 2022. The Author(s).
Conflict of interest statement
None of the authors has declared a conflict of interest.
Figures
Similar articles
-
Performance of a guideline-recommended algorithm for prognostication of poor neurological outcome after cardiac arrest.Intensive Care Med. 2020 Oct;46(10):1852-1862. doi: 10.1007/s00134-020-06080-9. Epub 2020 Jun 3. Intensive Care Med. 2020. PMID: 32494928 Free PMC article.
-
Does a combination of ≥2 abnormal tests vs. the ERC-ESICM stepwise algorithm improve prediction of poor neurological outcome after cardiac arrest? A post-hoc analysis of the ProNeCA multicentre study.Resuscitation. 2021 Mar;160:158-167. doi: 10.1016/j.resuscitation.2020.12.003. Epub 2020 Dec 15. Resuscitation. 2021. PMID: 33338571
-
2021 European Resuscitation Council/European Society of Intensive Care Medicine Algorithm for Prognostication of Poor Neurological Outcome After Cardiac Arrest-Can Entry Criteria Be Broadened?Crit Care Med. 2024 Apr 1;52(4):531-541. doi: 10.1097/CCM.0000000000006113. Epub 2023 Dec 7. Crit Care Med. 2024. PMID: 38059722
-
Prognostication of neurologic outcome in cardiac arrest patients after mild therapeutic hypothermia: a meta-analysis of the current literature.Intensive Care Med. 2013 Oct;39(10):1671-82. doi: 10.1007/s00134-013-3004-y. Epub 2013 Jun 26. Intensive Care Med. 2013. PMID: 23801384 Review.
-
Intensive care medicine research agenda on cardiac arrest.Intensive Care Med. 2017 Sep;43(9):1282-1293. doi: 10.1007/s00134-017-4739-7. Epub 2017 Mar 11. Intensive Care Med. 2017. PMID: 28285322 Review.
Cited by
-
Cortical somatosensory evoked potential amplitudes and clinical outcome after cardiac arrest: a retrospective multicenter study.J Neurol. 2023 Dec;270(12):5999-6009. doi: 10.1007/s00415-023-11951-4. Epub 2023 Aug 28. J Neurol. 2023. PMID: 37639017 Free PMC article.
-
Use of Prognostication Instruments in Prognostication Procedures of Postanoxic Coma Patients over Time: A Retrospective Study.J Clin Med. 2023 May 9;12(10):3357. doi: 10.3390/jcm12103357. J Clin Med. 2023. PMID: 37240462 Free PMC article.
-
Quantitative analysis of apparent diffusion coefficients to predict neurological prognosis in cardiac arrest survivors: an observational derivation and internal-external validation study.Crit Care. 2024 Apr 25;28(1):138. doi: 10.1186/s13054-024-04909-z. Crit Care. 2024. PMID: 38664807 Free PMC article.
-
Prognostic accuracy of head computed tomography for prediction of functional outcome after out-of-hospital cardiac arrest: Rationale and design of the prospective TTM2-CT-substudy.Resusc Plus. 2022 Oct 12;12:100316. doi: 10.1016/j.resplu.2022.100316. eCollection 2022 Dec. Resusc Plus. 2022. PMID: 36267356 Free PMC article.
-
Quantitative pupillometry for neuroprognostication in comatose post-cardiac arrest patients: A protocol for a predefined sub-study of the Blood pressure and Oxygenations Targets after Out-of-Hospital Cardiac Arrest (BOX)-trial.Resusc Plus. 2023 Sep 26;16:100475. doi: 10.1016/j.resplu.2023.100475. eCollection 2023 Dec. Resusc Plus. 2023. PMID: 37779885 Free PMC article.
References
-
- Lemiale V, Dumas F, Mongardon N, Giovanetti O, Charpentier J, Chiche JD, Carli P, Mira JP, Nolan J, Cariou A. Intensive care unit mortality after cardiac arrest: the relative contribution of shock and brain injury in a large cohort. Intensive Care Med. 2013;39:1972–1980. doi: 10.1007/s00134-013-3043-4. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
