

Microvascular Decompression for Trigeminal Neuralgia Caused by Venous Offending on the Ventral Side of the Root Entrance/Exit Zone: Classification and Management Strategy
- PMID: 35401405
- PMCID: PMC8990805
- DOI: 10.3389/fneur.2022.864061
Microvascular Decompression for Trigeminal Neuralgia Caused by Venous Offending on the Ventral Side of the Root Entrance/Exit Zone: Classification and Management Strategy
Abstract
Background: Trigeminal neuralgia (TGN) is typically caused by an offending artery (OA) but may also involve an offending vein. Venous offending on the ventral side of the root entrance/exit zone (VO-VREZ) is particularly challenging.
Objective: To analyze the rate and pattern of VO-VREZ and propose management strategy accordingly.
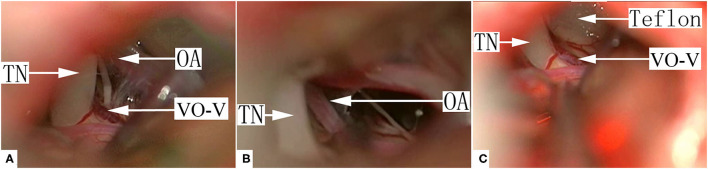
Methods: VO-VREZ was classified into 3 types based on its anatomical relationship with a nerve root (A, the vein was covered by the nerve root entirely; B, the vein was lateral to the nerve root; and C, the vein penetrated the nerve root) and 3 groups based on the absence/presence of offending artery (I, no OA; II, suspected OA; and III, definitive OA).
Results: The analysis included 143 cases with complete follow-up. Type A, B, and C accounted for 11.9, 31.5, and 56.6% of the cases, respectively. Group I, II, and III accounted for 24.5, 26.6, and 49.0%, respectively. Most group I VO-VREZ cases (26 out of 31) were managed with coagulation followed by division. Most group II VO-VREZ cases (31 out of 38) were decompressed with shredded Teflon interposition. Group III VO-VREZ was left in place in all 70 cases. Immediate pain relief was achieved in all cases. Temporary hemifacial hypesthesia occurred in 21 patients (14.7%), among which 14 were managed with Teflon decompression. Within the 4.5-year median follow-up, pain recurred in 11 patients (7.7%), but all with lesser intensity.
Conclusion: VO-VREZ is not uncommon in patients with TGN. Different management strategy should be chosen according to the anatomical feature and the absence/presence of arterial conflict.
Keywords: microvascular decompression; offending artery; offending vein; root entrance/exit zone; trigeminal neuralgia.
Copyright © 2022 Wang, Yu, Kwok, Wang and Yin.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures






Similar articles
-
Treatment Strategies for Different Types of Intraneural Offending Vessels in Microvascular Decompression Surgery for Trigeminal Neuralgia: An Analytic Report of 58 Cases.Neurosurgery. 2022 May 1;90(5):562-568. doi: 10.1227/neu.0000000000001877. Neurosurgery. 2022. PMID: 35175236
-
Characteristics and management of the offending veins in microvascular decompression surgery for trigeminal neuralgia.Neurosurg Rev. 2021 Aug;44(4):2337-2347. doi: 10.1007/s10143-020-01411-2. Epub 2020 Oct 27. Neurosurg Rev. 2021. PMID: 33111206 Free PMC article.
-
Microvascular Decompression for Trigeminal Neuralgia: Zone Exploration and Decompression Techniques.J Craniofac Surg. 2015 Nov;26(8):2381-4. doi: 10.1097/SCS.0000000000002147. J Craniofac Surg. 2015. PMID: 26501973
-
Atrophic changes in the trigeminal nerves of patients with trigeminal neuralgia due to neurovascular compression and their association with the severity of compression and clinical outcomes.J Neurosurg. 2014 Jun;120(6):1484-95. doi: 10.3171/2014.2.JNS131288. Epub 2014 Apr 18. J Neurosurg. 2014. PMID: 24745706
-
Trigeminal Neuralgia Attributable to Intraneural Trigeminocerebellar Artery: Case Report and Review of the Literature.World Neurosurg. 2016 Apr;88:687.e7-687.e11. doi: 10.1016/j.wneu.2015.11.059. Epub 2015 Dec 20. World Neurosurg. 2016. PMID: 26714300 Review.
Cited by
-
Delayed pain relief in patients with trigeminal neuralgia following microvascular decompression: A single-central retrospective study.Front Neurol. 2022 Oct 19;13:946897. doi: 10.3389/fneur.2022.946897. eCollection 2022. Front Neurol. 2022. PMID: 36341100 Free PMC article.
-
Surgical and Clinical Outcomes of Microvascular Decompression: A Comparative Study between Young and Elderly Patients.Brain Sci. 2022 Sep 9;12(9):1216. doi: 10.3390/brainsci12091216. Brain Sci. 2022. PMID: 36138952 Free PMC article.
-
Chiari malformation and its influence on trigeminal neuralgia: a systematic review.Ann Med Surg (Lond). 2024 Sep 4;86(10):5999-6011. doi: 10.1097/MS9.0000000000002527. eCollection 2024 Oct. Ann Med Surg (Lond). 2024. PMID: 39359841 Free PMC article. Review.
References
-
- Dandy WE. Concerning the cause of trigeminal neuralgia. Am J Surg. (1934) 24:447–55. 10.1016/S0002-9610(34)90403-7 - DOI
LinkOut - more resources
Full Text Sources
Miscellaneous