

Development of Potent Cellular and Humoral Immune Responses in Long-Term Hemodialysis Patients After 1273-mRNA SARS-CoV-2 Vaccination
- PMID: 35401504
- PMCID: PMC8983822
- DOI: 10.3389/fimmu.2022.845882
Development of Potent Cellular and Humoral Immune Responses in Long-Term Hemodialysis Patients After 1273-mRNA SARS-CoV-2 Vaccination
Abstract
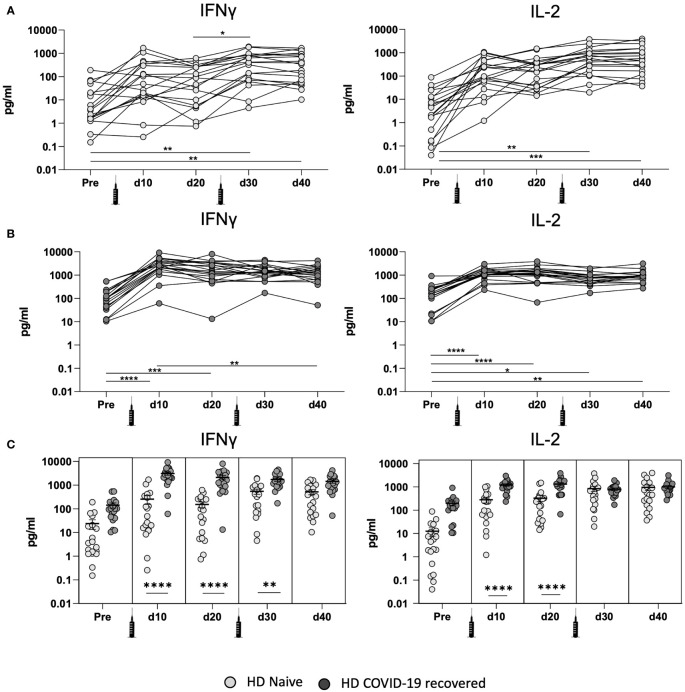
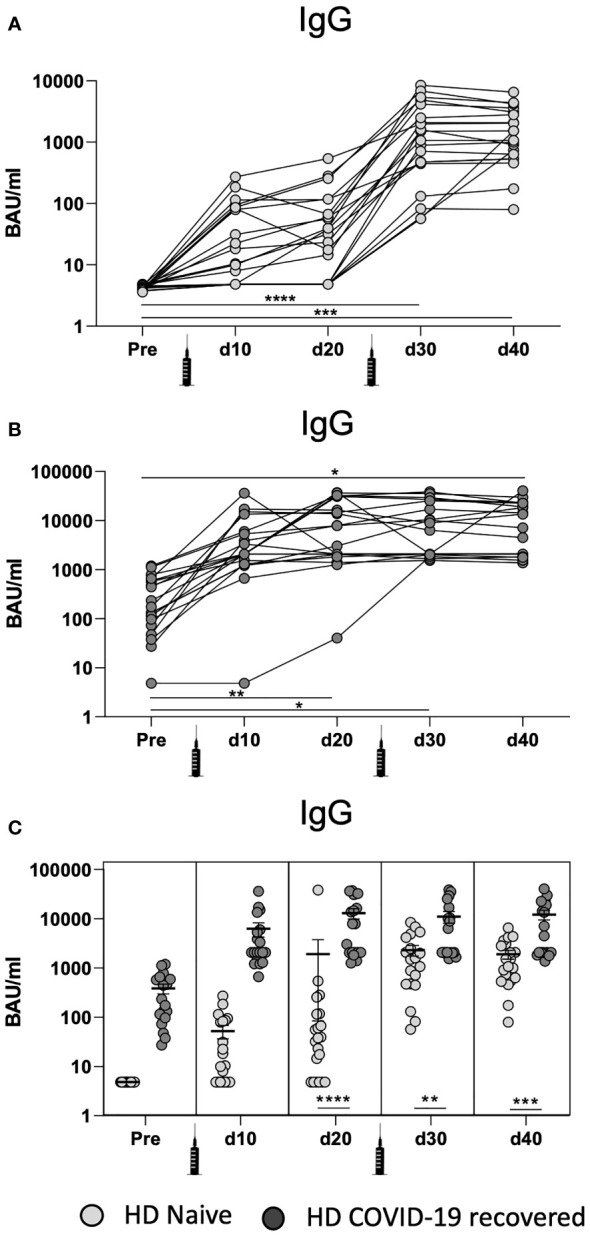
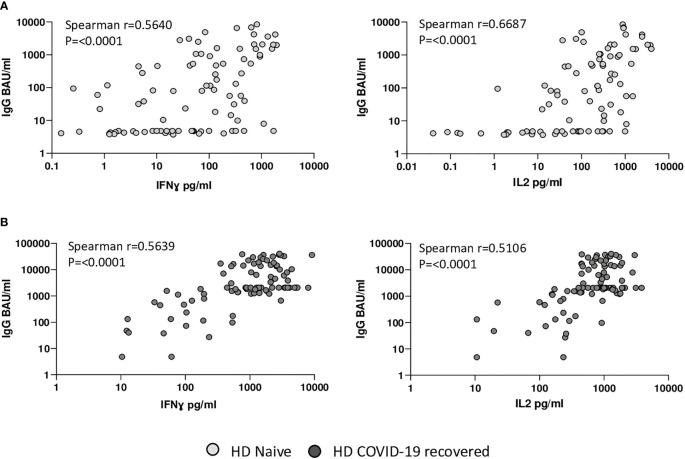
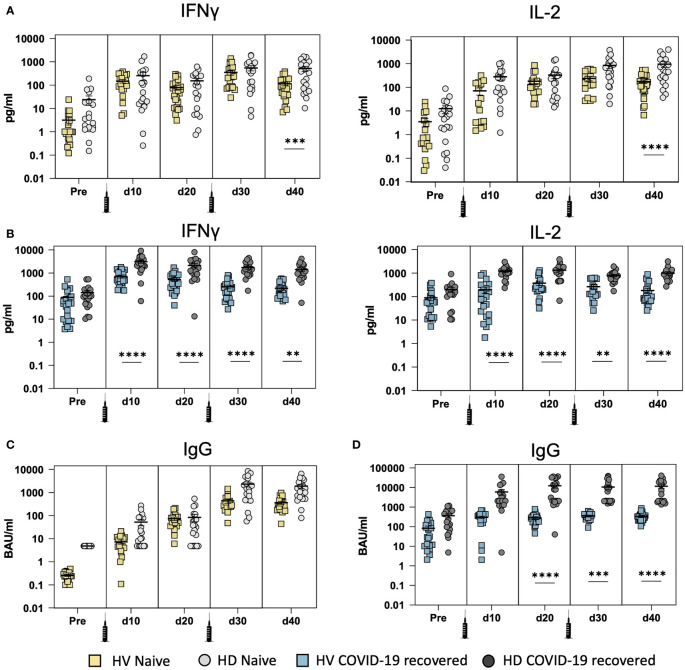
Long-term hemodialysis (HD) patients are considered vulnerable and at high-risk of developing severe acute respiratory syndrome coronavirus type 2 (SARS-CoV-2) infection due to their immunocompromised condition. Since COVID-19 associated mortality rates are higher in HD patients, vaccination is critical to protect them. The response towards vaccination against COVID-19 in HD patients is still uncertain and, in particular the cellular immune response is not fully understood. We monitored the humoral and cellular immune responses by analysis of the serological responses and Spike-specific cellular immunity in COVID-19-recovered and naïve HD patients in a longitudinal study shortly after vaccination to determine the protective effects of 1273-mRNA vaccination against SARS-CoV-2 in these high-risk patients. In naïve HD patients, the cellular immune response measured by IL-2 and IFN-ɣ secretion needed a second vaccine dose to significantly increase, with a similar pattern for the humoral response. In contrast, COVID-19 recovered HD patients developed a potent and rapid cellular and humoral immune response after the first vaccine dose. Interestingly, when comparing COVID-19 recovered healthy volunteers (HV), previously vaccinated with BNT162b2 vaccine to HD patients vaccinated with 1273-mRNA, these exhibited a more robust immune response that is maintained longitudinally. Our results indicate that HD patients develop strong cellular and humoral immune responses to 1273-mRNA vaccination and argue in favor of personalized immune monitoring studies in HD patients, especially if COVID-19 pre-exposed, to adapt COVID-19 vaccination protocols for this immunocompromised population.
Keywords: COVID-19; SARS-CoV-2 vaccine; cellular response; chronic kidney disease; hemodialysis; humoral response.
Copyright © 2022 Gonzalez-Perez, Montes-Casado, Conde, Cervera, Baranda, Berges-Buxeda, Perez-Olmeda, Sanchez-Tarjuelo, Utrero-Rico, Lozano-Ojalvo, Torre, Schwarz, Guccione, Camara, Llópez-Carratalá, Gonzalez-Parra, Portoles, Ortiz, Portoles and Ochando.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Sánchez-Álvarez JE, Pérez Fontán M, Jiménez Martín C, Blasco Pelícano M, Cabezas Reina CJ, Sevillano Prieto ÁM, et al. SARS-CoV-2 Infection in Patients on Renal Replacement Therapy. Report of the COVID-19 Registry of the Spanish Society of Nephrology (SEN). Nefrologia (Engl Ed) (2020) 40(3):272–8. doi: 10.1016/j.nefro.2020.04.002 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous