

COVID-19-Associated Acute Asymmetric Hemorrhagic Necrotizing Encephalopathy: A Case Report
- PMID: 35401914
- PMCID: PMC8977755
- DOI: 10.1177/19418744211055360
COVID-19-Associated Acute Asymmetric Hemorrhagic Necrotizing Encephalopathy: A Case Report
Abstract
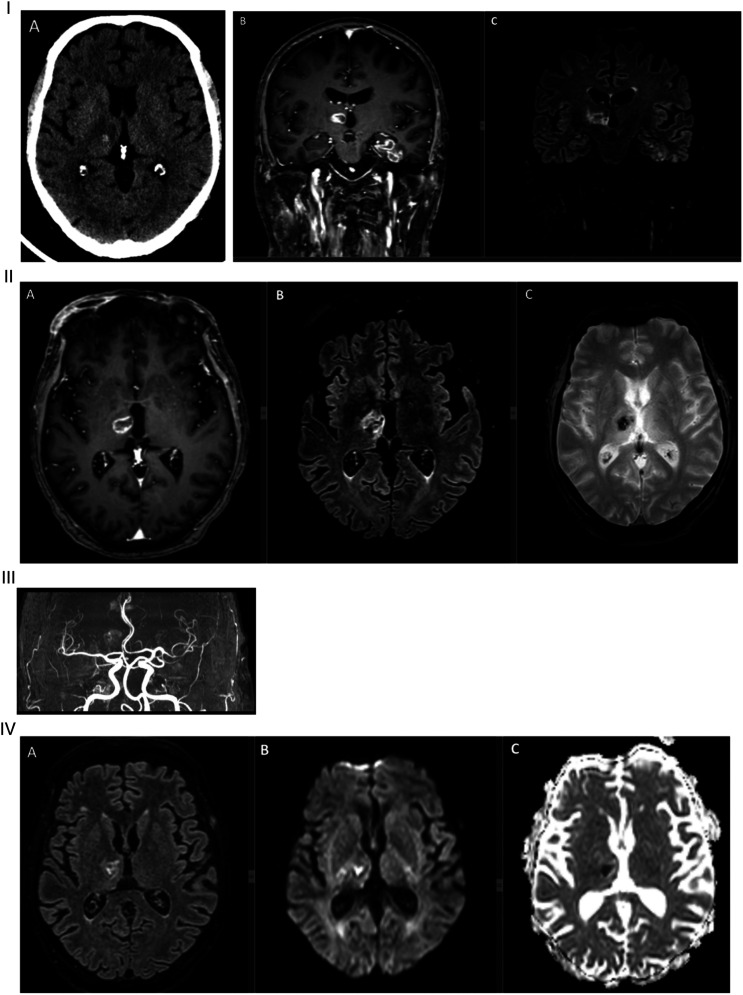
Background: Coronavirus disease 2019 (COVID-19) has been associated with many neurological complications affecting the central nervous system. Purpose: Our aim was to describe a case of COVID-19 associated with a probable variant of acute necrotizing encephalopathy (ANE). Results: A 60-year-old man who presented with a 3-day history of dyspnea, fever, and cough tested positive for severe acute respiratory syndrome-coronavirus 2 (SARS-CoV-2). Five days following his admission, the patient was intubated secondary to respiratory failure. Following his extubation 16 days later, he was found to have a left-sided weakness. Magnetic resonance imaging (MRI) of the brain showed hemorrhagic rim-enhancing lesions involving the right thalamus, left hippocampus, and left parahippocampal gyrus. These lesions showed decreased relative cerebral blood flow on MR perfusion and restricted on diffusion-weighted imaging. These neuroimaging findings were consistent with ANE. The left-sided weakness gradually improved over the subsequent weeks. Conclusions: We concluded that COVID-19 can be associated with ANE, a condition believed to be the result of an immune-mediated process with activation of the innate immune system. Future studies must address whether biological drugs targeting the pro-inflammatory cytokines could prevent the development of this condition.
Keywords: COVID-19; acute necrotizing encephalopathy; case report; magnetic resonance imaging.
© The Author(s) 2022.
Conflict of interest statement
Declaration of Conflicting Interests: The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures



Similar articles
-
A fatal case of COVID-19-associated acute necrotizing encephalopathy.Eur J Neurol. 2021 Nov;28(11):3870-3872. doi: 10.1111/ene.14966. Eur J Neurol. 2021. PMID: 34655265 Free PMC article.
-
Fatal Acute Necrotizing Encephalopathy in a 17-Year-Old Girl with COVID-19: A Case Report.Am J Case Rep. 2025 May 1;26:e946932. doi: 10.12659/AJCR.946932. Am J Case Rep. 2025. PMID: 40308025 Free PMC article.
-
MRI Findings of COVID-19 Associated Acute Necrotizing Encephalopathy in Two Pediatric Patients: Case Report and Literature Review.J Korean Soc Radiol. 2024 May;85(3):682-690. doi: 10.3348/jksr.2023.0023. Epub 2024 May 14. J Korean Soc Radiol. 2024. PMID: 38873375 Free PMC article.
-
Acute hemorrhagic leukoencephalitis in a COVID-19 patient-a case report with literature review.Neuroradiology. 2021 May;63(5):653-661. doi: 10.1007/s00234-021-02667-1. Epub 2021 Feb 11. Neuroradiology. 2021. PMID: 33575849 Free PMC article. Review.
-
Spectrum of Neurological Manifestations in Covid-19: A Review.Neurol India. 2020 May-Jun;68(3):560-572. doi: 10.4103/0028-3886.289000. Neurol India. 2020. PMID: 32643664 Review.
Cited by
-
COVID-19 related acute necrotizing encephalopathy presenting in the early postoperative period.Arch Clin Cases. 2023 Jun 7;10(2):78-85. doi: 10.22551/2023.39.1002.10246. eCollection 2023. Arch Clin Cases. 2023. PMID: 37293685 Free PMC article.
-
Acute Necrotizing Encephalopathy in Adult Patients With COVID-19: A Systematic Review of Case Reports and Case Series.J Clin Neurol. 2023 Nov;19(6):597-611. doi: 10.3988/jcn.2022.0431. Epub 2023 Jul 13. J Clin Neurol. 2023. PMID: 37455513 Free PMC article.
-
COVID-19: Unveiling the Neuropsychiatric Maze-From Acute to Long-Term Manifestations.Biomedicines. 2024 May 22;12(6):1147. doi: 10.3390/biomedicines12061147. Biomedicines. 2024. PMID: 38927354 Free PMC article. Review.
References
-
- Ito Y, Ichiyama T, Kimura H, et al. Detection of influenza virus RNA by reverse transcription‐PCR and proinflammatory cytokines in influenza‐virus‐associated encephalopathy. J Med Virol. 1999;58:420-425. - PubMed
-
- Yoshikawa H, Watanabe T, Abe T, et al. Clinical diversity in acute necrotizing encephalopathy. J Child Neurol. 1999;14:249-255. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous