

Deep Infiltrating Endometriosis Malignant Invasion of Cervical Wall and Rectal Wall With Lynch Syndrome: A Rare Case Report and Review of Literature
- PMID: 35402227
- PMCID: PMC8983876
- DOI: 10.3389/fonc.2022.832228
Deep Infiltrating Endometriosis Malignant Invasion of Cervical Wall and Rectal Wall With Lynch Syndrome: A Rare Case Report and Review of Literature
Abstract
Background: Malignant transformation of deep infiltrating endometriosis (DIE) invading the cervix and rectum is quite rare, especially in patients combined with Lynch syndrome (LS). We report a rare case of a 49-year-old perimenopausal woman with endometrioid carcinoma arising from the pouch of Douglas, invading the cervix and rectum 1 year after a unilateral salpingo-oophorectomy treatment for ovarian endometriosis. The genetic testing of the patient showed germline mutations in MSH2, which combined with the special family history of colorectal cancer of the patient, was also thought to be associated with LS. We have analyzed the reported cases of DIE malignant transformation over the last 10 years, and reviewed the relevant literature, in order to strengthen the clinical management of patients with endometriosis, particularly patients with DIE, and reveal a possible correlation between malignant transformation of endometriosis and LS.
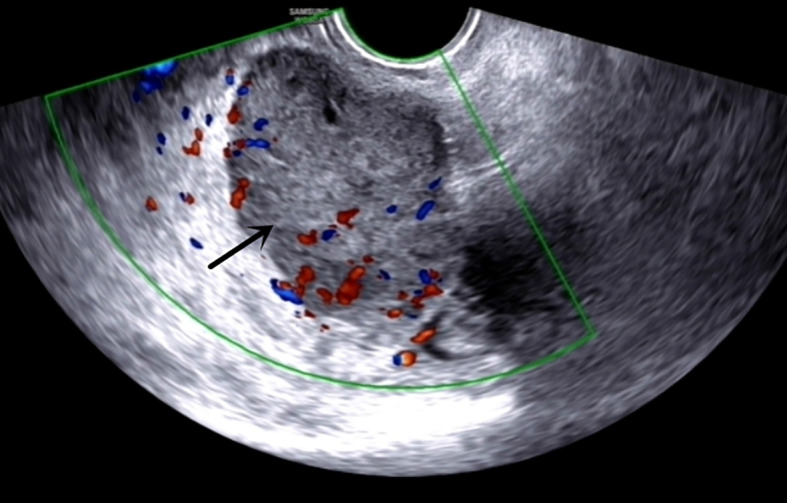
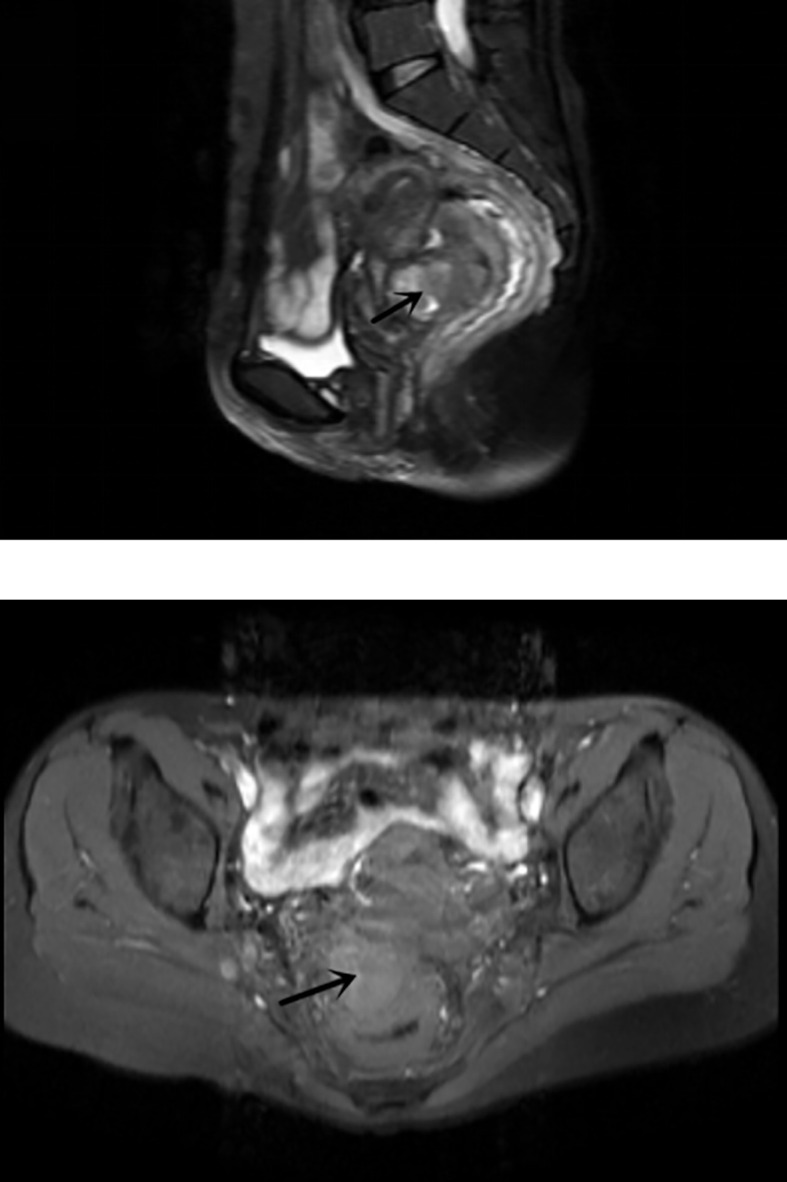
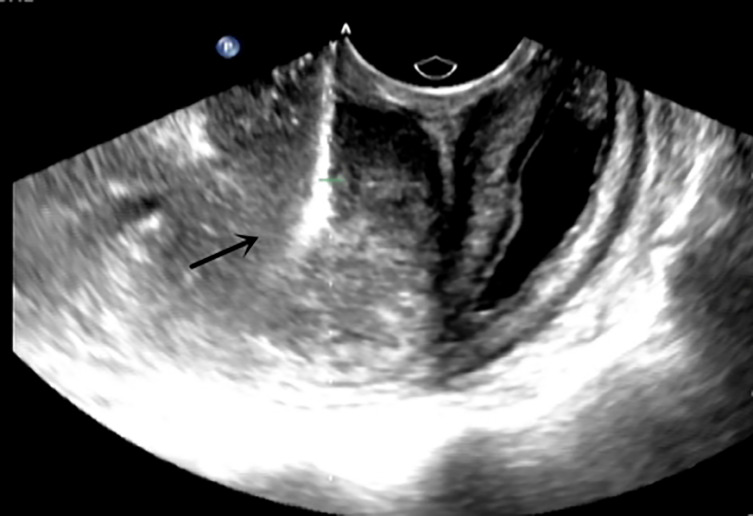
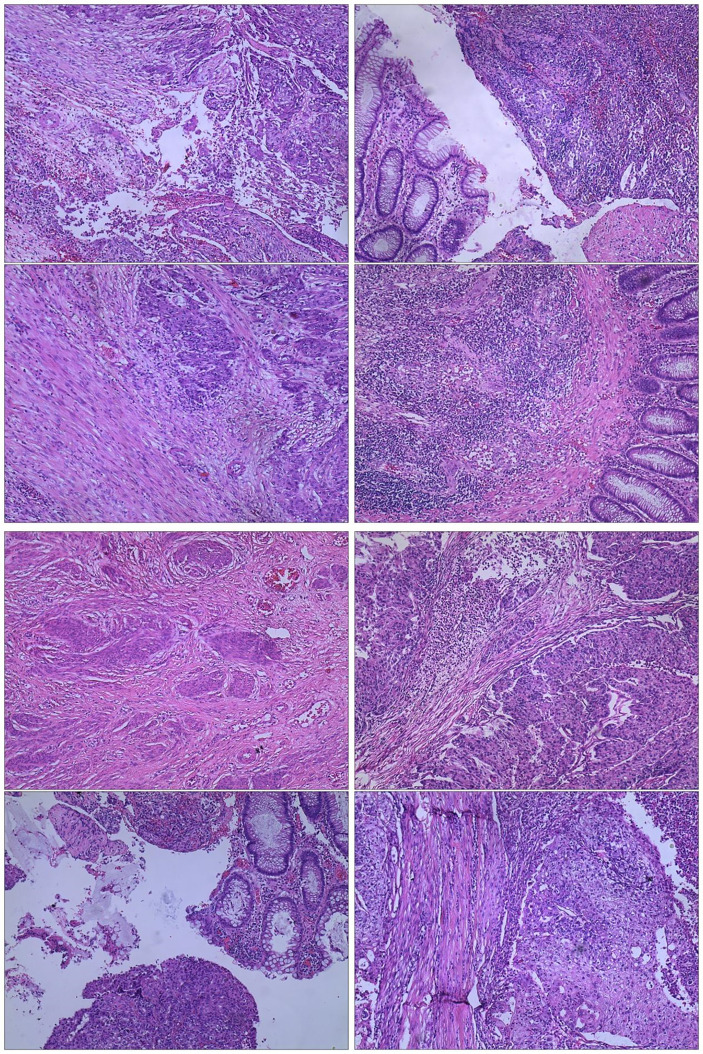
Case presentation: A 49-year-old perimenopausal woman presented with hypogastralgia, diarrhea, and intermittent fever for more than 1 month. A Transvaginal ultrasound (TVS) showed a cervix isthmus mass, and a magnetic resonance imaging (MRI) showed a mass in pouch of Douglas with high suspicion of malignancy, possibly invading the anterior wall of the rectum. Prior to surgery, the patient performed the ultrasound guided pelvic mass biopsy through the vagina, and the pathology of the mass showed endometrioid carcinoma. The patient received a gynecological-surgical laparotomy and enterostomy, and a histopathology revealed endometrioid carcinoma infiltrating the cervical wall and rectal wall. In the family genetic history of the patient, her mother and two sisters suffered from colorectal cancer, so lesion tissue and blood were taken for genetic testing, which showed a germline mutation in MSH2, with LS being considered. After the surgical treatment, the patient received six courses of paclitaxel-carboplatin chemotherapy. During the course of treatment, bone marrow suppression occurred, but was healed after symptomatic treatment. To date, the patient is generally in good health, and imaging examination showed no evidence of recurrence.
Conclusion: The risk of malignant transformation of endometriosis is increased in perimenopause and postmenopause, as DIE is a rare malignant transformation of endometriosis. DIE can invade other adjacent organs and cause poor prognosis, thus, comprehensive gynecological-surgical treatment should be necessary. In addition, if histopathology showed endometrioid carcinoma, the possibility of LS should be considered, and if necessary, immunohistochemical staining and gene detection should be improved to provide follow-up targeted therapy and immunotherapy.
Keywords: Lynch syndrome; deep infiltrating endometriosis; endometriosis; malignant transformation; malignant tumor.
Copyright © 2022 Li, Wang, Wang, Li and Liu.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Clinicopathological features of endometriosis‑associated adenocarcinoma of the rectum: A report of two cases.Oncol Lett. 2024 Aug 30;28(5):523. doi: 10.3892/ol.2024.14656. eCollection 2024 Nov. Oncol Lett. 2024. PMID: 39268170 Free PMC article.
-
Primary endometrioid carcinoma of the uterosacral ligament arising from deep infiltrating endometriosis 6 years after bilateral salpingo-oophorectomy due to atypical proliferative endometrioid tumor of the ovary: a rare case report.World J Surg Oncol. 2020 Dec 11;18(1):329. doi: 10.1186/s12957-020-02105-1. World J Surg Oncol. 2020. PMID: 33308243 Free PMC article.
-
Diaphragmatic clear cell carcinoma with Lynch syndrome after surgery for atypical endometrial hyperplasia and ovarian endometriosis: A case report.Mol Clin Oncol. 2024 May 16;21(1):46. doi: 10.3892/mco.2024.2744. eCollection 2024 Jul. Mol Clin Oncol. 2024. PMID: 38826696 Free PMC article.
-
Malignant transformation of hepatic endometriosis: a case report and literature review.BMC Womens Health. 2021 Jun 21;21(1):249. doi: 10.1186/s12905-021-01366-6. BMC Womens Health. 2021. PMID: 34154577 Free PMC article. Review.
-
Endometrioid adenocarcinoma of the rectovaginal septum with invasion of the rectum: a case report and review of literature.World J Surg Oncol. 2019 Dec 4;17(1):206. doi: 10.1186/s12957-019-1743-0. World J Surg Oncol. 2019. PMID: 31801560 Free PMC article. Review.
Cited by
-
Digestive system deep infiltrating endometriosis: What do we know.J Cell Mol Med. 2023 Dec;27(23):3649-3661. doi: 10.1111/jcmm.17921. Epub 2023 Aug 25. J Cell Mol Med. 2023. PMID: 37632165 Free PMC article. Review.
-
Clinicopathological features of endometriosis‑associated adenocarcinoma of the rectum: A report of two cases.Oncol Lett. 2024 Aug 30;28(5):523. doi: 10.3892/ol.2024.14656. eCollection 2024 Nov. Oncol Lett. 2024. PMID: 39268170 Free PMC article.
-
At what age endometriosis-associated ovarian cancer is diagnosed? The implications for women in the reproductive age.Front Oncol. 2023 May 23;13:1193123. doi: 10.3389/fonc.2023.1193123. eCollection 2023. Front Oncol. 2023. PMID: 37287920 Free PMC article. No abstract available.
-
High grade endometrioid carcinoma arising from deep infiltrating endometriosis extending deeply into the pelvis: a case report.J Surg Case Rep. 2025 May 23;2025(5):rjaf266. doi: 10.1093/jscr/rjaf266. eCollection 2025 May. J Surg Case Rep. 2025. PMID: 40417051 Free PMC article.
-
Case Series and a Literature Review: Two Ovarian Clear Cell Carcinoma Cases with Recurrent Endometriosis.Int J Womens Health. 2023 Oct 24;15:1611-1619. doi: 10.2147/IJWH.S418135. eCollection 2023. Int J Womens Health. 2023. PMID: 37901720 Free PMC article.
References
-
- Pearce CL, Templeman C, Rossing MA, Lee A, Near AM, Webb PM, et al. . Ovarian Cancer Association Consortium. Association Between Endometriosis and Risk of Histological Subtypes of Ovarian Cancer: A Pooled Analysis of Case-Control Studies. Lancet Oncol (2012) 13(4):385–94. doi: 10.1016/S1470-2045(11)70404-1 - DOI - PMC - PubMed
-
- Samartzis EP, Labidi-Galy SI, Moschetta M, Uccello M, Kalaitzopoulos DR, Perez-Fidalgo JA, et al. . Endometriosis-Associated Ovarian Carcinomas: Insights Into Pathogenesis, Diagnostics, and Therapeutic Targets-A Narrative Review. Ann Transl Med (2020) 8(24):1712. doi: 10.21037/atm-20-3022a - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources