

New Technique of Laparoscopic Paraaortic Lymph Node Dissection for Colorectal Cancer Using Fluorescence Navigation
- PMID: 35403145
- PMCID: PMC8988955
- DOI: 10.21873/cdp.10042
New Technique of Laparoscopic Paraaortic Lymph Node Dissection for Colorectal Cancer Using Fluorescence Navigation
Abstract
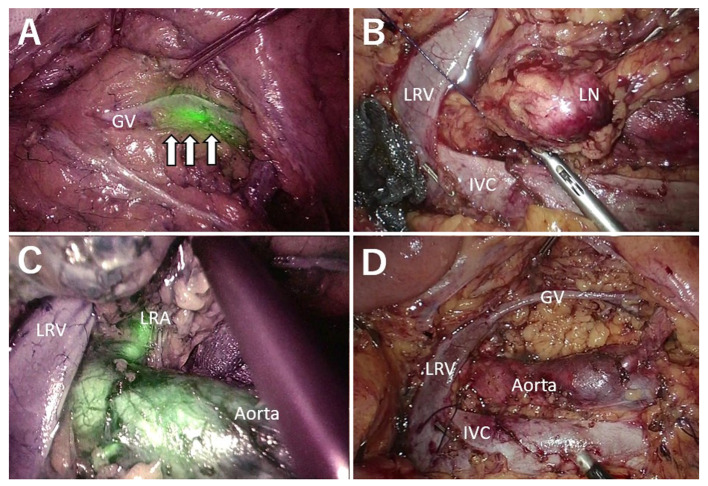
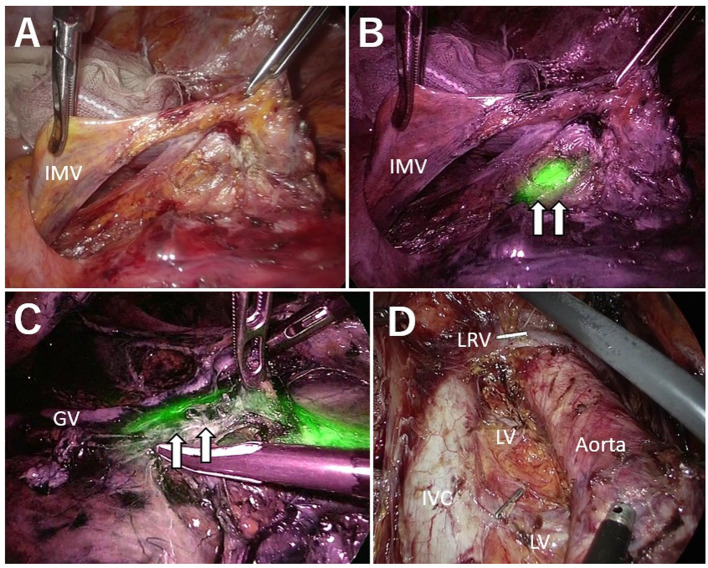
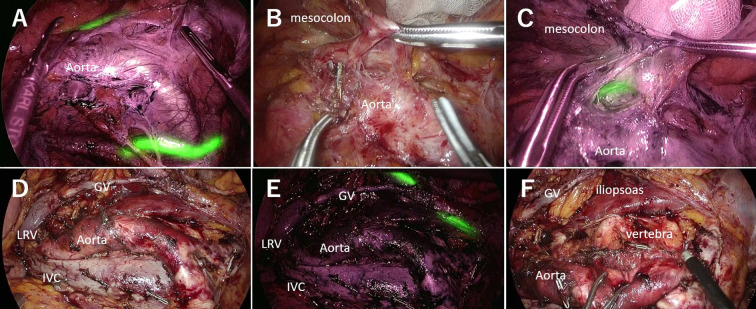
Background/aim: According to limited current reports, therapeutic paraaortic lymph node (PALN) dissection with intensive combined therapy for colorectal cancer improves prognosis in select patients. Laparoscopic PALN dissection is a difficult technique that has not yet been established. We applied this procedure using an intraoperative fluorescence navigation technique with a near-infrared ray catheter (NIRC™) fluorescent ureteral catheter (NIRFUC).
Patients and methods: We evaluated the utility of laparoscopic fluorescence navigation and the short-term outcomes of 6 patients undergoing laparoscopic PALN dissection.
Results: There were 3 surgeries for synchronous metastasis and 3 surgeries for recurrent metastasis. The mean surgical duration, blood loss, and postoperative hospital stay were 677 (range=518-1,090) min, 7.5 (range=3-1,600) ml, and 14 (range=9-33) days, respectively. Postoperative complications (Clavien-Dindo grade >III) occurred in 1 case.
Conclusion: Dissection around the ureter was navigated with a NIRFUC. Fluorescence ureteral navigation facilitated completion of the complex laparoscopic PALN dissection procedure.
Keywords: Laparoscopic surgery; colorectal cancer; fluorescence navigation; paraaortic lymph node dissection; ureter.
Copyright 2021, International Institute of Anticancer Research.
Conflict of interest statement
Shunjin Ryu MD, PhD, Keigo Hara MD, Keisuke Goto MD, Keisuke Goto MD, Atsuko Okamoto MD, Takahiro Kitagawa MD, Rui Marukuchi MD, PhD, Ryusuke Ito MD, PhD, and Yukio Nakabayashi MD, PhD have no conflicts of interest or financial ties to disclose in relation to this study.
Figures
References
-
- Howlader N, Noone AM, Krapcho M, Miller D, Bishop K, Kosary CL, Yu M, Ruhl J, Tatalovich Z, Mariotto A, Lewis DR, Chen HS, Feuer EJ, Cronin KA. Seer cancer statistics review, 1975-2014. Bethesda, MD, National Cancer Institute. Available at: https://seer.cancer.gov/archive/csr/1975_2014/ [Last accessed on June 14, 2021]
LinkOut - more resources
Full Text Sources