

A real-world, observational study of erenumab for migraine prevention in Canadian patients
- PMID: 35403223
- PMCID: PMC9320807
- DOI: 10.1111/head.14291
A real-world, observational study of erenumab for migraine prevention in Canadian patients
Abstract
Objectives: To assess real-world effectiveness, safety, and usage of erenumab in Canadian patients with episodic and chronic migraine with prior ineffective prophylactic treatments.
Background: In randomized controlled trials, erenumab demonstrated efficacy for migraine prevention in patients with ≤4 prior ineffective prophylactic migraine therapies. The "Migraine prevention with AimoviG: Informative Canadian real-world study" (MAGIC) assessed real-world effectiveness of erenumab in Canadian patients with migraine.
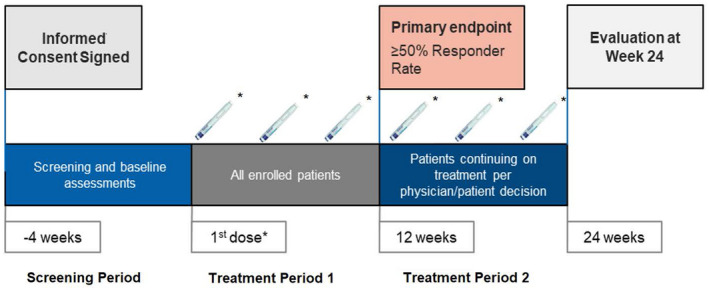
Methods: MAGIC was a prospective open-label, observational study conducted in Canadian patients with chronic migraine (CM) and episodic migraine (EM) with two to six categories of prior ineffective prophylactic therapies. Participants were administered 70 mg or 140 mg erenumab monthly based on physician's assessment. Migraine attacks were self-assessed using an electronic diary and patient-reported outcome questionnaires. The primary outcome was the proportion of subjects achieving ≥50% reduction in monthly migraine days (MMD) after the 3-month treatment period.
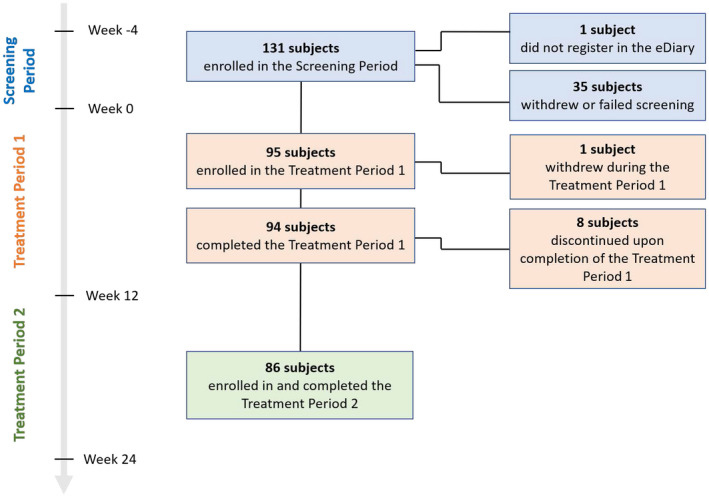
Results: Among the 95 participants who mostly experienced two (54.7%) or three (32.6%) prior categories of ineffective prophylactic therapies and who initiated erenumab, treatment was generally safe and well tolerated; 89/95 (93.7%) participants initiated treatment with 140 mg erenumab. At week 12, 32/95 (33.7%) participants including 17/64 (26.6%) CM and 15/32 (48.4%) EM achieved ≥50% reduction in MMD while 30/86 (34.9%) participants including 19/55 (34.5%) CM and 11/31 (35.5%) EM achieved ≥50% reduction in MMD at week 24. Through patient-reported outcome questionnaires, 62/95 (65.3%) and 45/86 (52.3%) participants reported improvement of their condition at weeks 12 and 24, respectively. Physicians observed improvement in the condition of 78/95 (82.1%) and 67/86 (77.9%) participants at weeks 12 and 24, respectively.
Conclusion: One-third of patients with EM and CM achieved ≥50% MMD reduction after 3 months of erenumab treatment. This study provides real-world evidence of erenumab effectiveness, safety, and usage for migraine prevention in adult Canadian patients with multiple prior ineffective prophylactic treatments.
Keywords: chronic migraine; effectiveness; episodic migraine; erenumab; real-world.
© 2022 Novartis Pharmaceuticals Canada Inc. Headache: The Journal of Head and Face Pain published by Wiley Periodicals LLC on behalf of American Headache Society.
Conflict of interest statement
Novartis Pharmaceuticals Canada Inc. funded the study. The sponsor was involved in the design, interpretation, and reporting of study results. AA and GSP were full‐time employees of IQVIA Solutions Canada Inc. at the time of the study. JKM and JM are full‐time employees of IQVIA Solutions Canada Inc. DR, AF, and NB are full‐time employees of Novartis Pharmaceuticals Canada Inc. WJB has served on medical advisory boards or received speaker honoraria from Allergan, Novartis Pharmaceuticals Inc., Weber and Weber, Teva, Eli Lilly, and Lundbeck. SS has received speaker honoraria from Abbvie, Miravo, Novartis Pharmaceuticals Inc., Teva, Eli Lilly, and Lundbeck. RG has served on medical advisory boards or received speaker honoraria from Allergan, Novartis Pharmaceuticals Inc., Teva, Eli Lilly, and Lundbeck. EL, JG, and SC have received consultation fees from Novartis Pharmaceuticals Inc.
Figures
References
-
- Dodick DW. Migraine. Lancet. 2018;391:1315‐1330. - PubMed
-
- Blumenfeld AM, Bloudek LM, Becker WJ, et al. Patterns of use and reasons for discontinuation of prophylactic medications for episodic migraine and chronic migraine: results from the second international burden of migraine study (IBMS‐II). Headache. 2013;53:644‐655. - PubMed
-
- Zimmermann U, Fischer JA, Frei K, Fischer AH, Reinscheid RK, Muff R. Identification of adrenomedullin receptors in cultured rat astrocytes and in neuroblastboma x glioma hybrid cells (NG108‐15). Brain Res. 1996;724:238‐245. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
