

Retrospective Evaluation of Various Serological Assays and Multiple Parameters for Optimal Diagnosis of Lyme Neuroborreliosis in a Routine Clinical Setting
- PMID: 35404103
- PMCID: PMC9241602
- DOI: 10.1128/spectrum.00061-22
Retrospective Evaluation of Various Serological Assays and Multiple Parameters for Optimal Diagnosis of Lyme Neuroborreliosis in a Routine Clinical Setting
Abstract
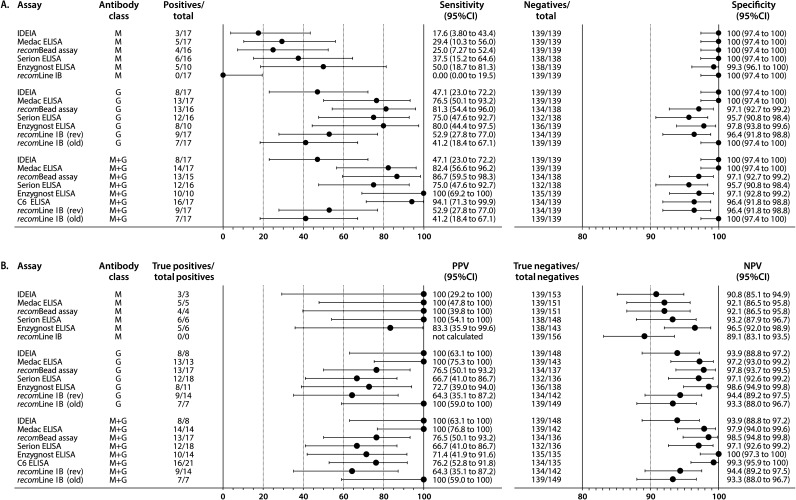
Laboratory diagnosis of Lyme neuroborreliosis (LNB) is challenging, and validated diagnostic algorithms are lacking. Therefore, this retrospective cross-sectional study aimed to compare the diagnostic performance of seven commercial antibody assays for LNB diagnosis. Random forest (RF) modeling was conducted to investigate whether the diagnostic performance using the antibody assays could be improved by including several routine cerebrospinal fluid (CSF) parameters (i.e., leukocyte count, total protein, blood-CSF barrier functionality, and intrathecal total antibody synthesis), two-tier serology on serum, the CSF level of the B-cell chemokine (C-X-C motif) ligand 13 (CXCL13), and a Borrelia species PCR on CSF. In total, 156 patients were included who were classified as definite LNB (n = 10), possible LNB (n = 7), or non-LNB patient (n = 139) according to the criteria of the European Federation of Neurological Societies using a consensus strategy for intrathecal Borrelia-specific antibody synthesis. The seven antibody assays showed sensitivities ranging from 47.1% to 100% and specificities ranging from 95.7% to 100%. RF modeling demonstrated that the sensitivities of most antibody assays could be improved by including other parameters to the diagnostic repertoire for diagnosing LNB (range: 94.1% to 100%), although with slightly lower specificities (range: 92.8% to 96.4%). The most important parameters for LNB diagnosis are the detection of intrathecally produced Borrelia-specific antibodies, two-tier serology on serum, CSF-CXCL13, Reibergram classification, and pleocytosis. In conclusion, this study shows that LNB diagnosis is best supported using multiparameter analysis. Furthermore, a collaborative prospective study is proposed to investigate if a standardized diagnostic algorithm can be developed for improved LNB diagnosis. IMPORTANCE The diagnosis of LNB is established by clinical symptoms, pleocytosis, and proof of intrathecal synthesis of Borrelia-specific antibodies. Laboratory diagnosis of LNB is challenging, and validated diagnostic algorithms are lacking. Therefore, this retrospective cross-sectional study aimed to compare the diagnostic performance of seven commercial antibody assays for LNB diagnosis. Multiparameter analysis was conducted to investigate whether the diagnostic performance using the antibody assays could be improved by including several routine (CSF) parameters. The results of this study show that LNB diagnosis is best supported using the detection of intrathecally produced Borrelia-specific antibodies, two-tier serology on serum, CSF-CXCL13, Reibergram classification, and pleocytosis. Furthermore, we propose a collaborative prospective study to investigate the potential role of constructing a diagnostic algorithm using multiparameter analysis for improved LNB diagnosis.
Keywords: Borrelia; Lyme neuroborreliosis; Reibergram; antibody index; cerebrospinal fluid; intrathecal antibody synthesis; multiparameter analysis; random forest; two-tier serology.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Enkelmann J, Bohmer M, Fingerle V, Siffczyk C, Werber D, Littmann M, Merbecks SS, Helmeke C, Schroeder S, Hell S, Schlotthauer U, Burckhardt F, Stark K, Schielke A, Wilking H. 2018. Incidence of notified Lyme borreliosis in Germany, 2013–2017. Sci Rep 8:14976. doi: 10.1038/s41598-018-33136-0. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
