

Helicobacter pylori Infection, Its Laboratory Diagnosis, and Antimicrobial Resistance: a Perspective of Clinical Relevance
- PMID: 35404105
- PMCID: PMC9491184
- DOI: 10.1128/cmr.00258-21
Helicobacter pylori Infection, Its Laboratory Diagnosis, and Antimicrobial Resistance: a Perspective of Clinical Relevance
Abstract
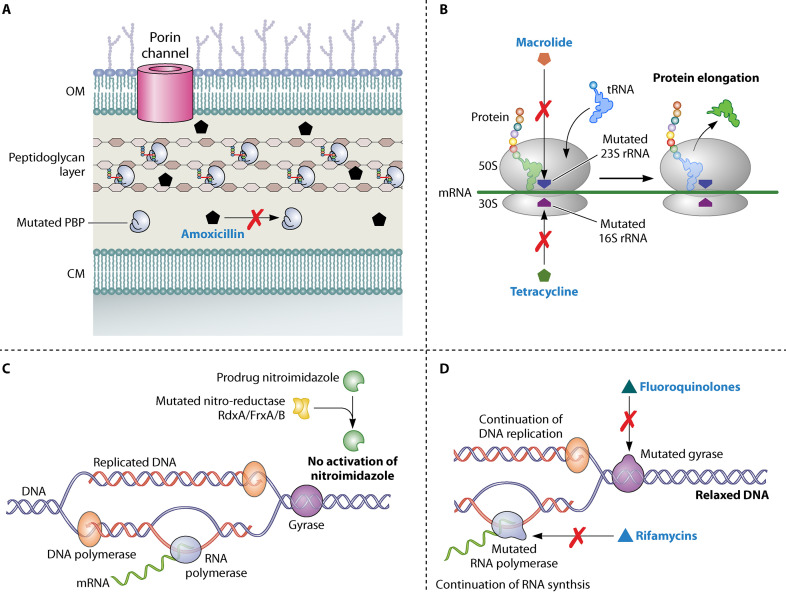
Despite the recent decrease in overall prevalence of Helicobacter pylori infection, morbidity and mortality rates associated with gastric cancer remain high. The antimicrobial resistance developments and treatment failure are fueling the global burden of H. pylori-associated gastric complications. Accurate diagnosis remains the opening move for treatment and eradication of infections caused by microorganisms. Although several reports have been published on diagnostic approaches for H. pylori infection, most lack the data regarding diagnosis from a clinical perspective. Therefore, we provide an intensive, comprehensive, and updated description of the currently available diagnostic methods that can help clinicians, infection diagnosis professionals, and H. pylori researchers working on infection epidemiology to broaden their understanding and to select appropriate diagnostic methods. We also emphasize appropriate diagnostic approaches based on clinical settings (either clinical diagnosis or mass screening), patient factors (either age or other predisposing factors), and clinical factors (either upper gastrointestinal bleeding or partial gastrectomy) and appropriate methods to be considered for evaluating eradication efficacy. Furthermore, to cope with the increasing trend of antimicrobial resistance, a better understanding of its emergence and current diagnostic approaches for resistance detection remain inevitable.
Keywords: Helicobacter pylori; RT-PCR; antimicrobial resistance; laboratory diagnosis; rapid urease test; stool antigen test; urea breath test.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- ARC Working Group. 1994. World Health Organization, International Agency for Research on Cancer. Schistosomes, liver flukes and Helicobacter pylori. WHO, Lyon, France.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
