

Feline Femoral Fracture Fixation: What are the options?
- PMID: 35404170
- PMCID: PMC11104039
- DOI: 10.1177/1098612X221090391
Feline Femoral Fracture Fixation: What are the options?
Abstract
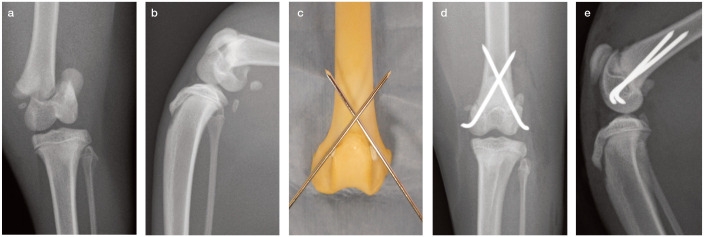
Practical relevance: The femur is the most commonly fractured bone in cats. Femoral fractures usually result from high-velocity trauma such as a road traffic accident or fall from a height and, as such, are associated with a wide variety of concurrent injuries. The initial focus of treatment should always be on assessment and stabilisation of the major body systems. Once any concurrent injuries have been addressed, all femoral fractures need surgical stabilisation, with the notable exception of greenstick fractures in very young cats, which can heal with cage rest alone. A number of different surgical options are available depending on the fracture type, location, equipment, surgeon experience and owner finances.
Clinical challenges: Femoral fractures can vary hugely in complexity and the small size of feline bones can limit the choice of implants. Furthermore, cats can present unique challenges in the postoperative period due to their active nature and the limited means to control their exercise level.
Audience: This review is aimed at general and feline-specific practitioners who have some experience of feline orthopaedics, as well as those simply wishing to expand their knowledge.
Aims: The aim of this review is to help clinicians assess, plan and manage feline femoral fractures. It provides an overview of diagnostic imaging and a discussion of a range of suitable surgical options, including the principles of different types of fixation. It also highlights cat-specific issues, approaches and implants pertinent to the management of these cases.
Evidence base: A number of original articles and textbook chapters covering many aspects of femoral fractures in cats and dogs have been published. Where possible, this review draws on information from key feline research and, where necessary, extrapolates from relevant canine literature. The authors also offer practical guidance based on their own clinical experience.
Keywords: Femur; capital femoral physis; distal femoral physis; femoral; fracture; trauma.
Conflict of interest statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and / or publication of this article.
Figures






















Similar articles
-
Analysis of feline humeral fracture morphology and a comparison of fracture repair stabilisation methods: 101 cases (2009-2020).J Feline Med Surg. 2022 Jun;24(6):e19-e27. doi: 10.1177/1098612X221080600. Epub 2022 Mar 7. J Feline Med Surg. 2022. PMID: 35254143 Free PMC article.
-
Use of veterinary interlocking nails for diaphyseal fractures in dogs and cats: 121 cases.Vet Surg. 2003 Jan-Feb;32(1):8-20. doi: 10.1053/jvet.2003.50008. Vet Surg. 2003. PMID: 12520485
-
Feline Diaphyseal Fractures: Management and treatment options.J Feline Med Surg. 2022 Jul;24(7):662-674. doi: 10.1177/1098612X221106354. J Feline Med Surg. 2022. PMID: 35775308 Free PMC article. Review.
-
The biomechanical properties of the feline femur.Vet Comp Orthop Traumatol. 2008;21(4):312-7. doi: 10.3415/vcot-07-08-0077. Vet Comp Orthop Traumatol. 2008. PMID: 18704236
-
Treatments for feline long bone fractures.Vet Clin North Am Small Anim Pract. 2002 Jul;32(4):927-47. doi: 10.1016/s0195-5616(02)00025-6. Vet Clin North Am Small Anim Pract. 2002. PMID: 12148319 Review.
Cited by
-
Fracture of the greater trochanter of the femur in 17 cats: imaging, clinical features and concurrent injuries.J Feline Med Surg. 2025 Apr;27(4):1098612X241305918. doi: 10.1177/1098612X241305918. Epub 2025 Apr 3. J Feline Med Surg. 2025. PMID: 40176569 Free PMC article.
-
Finite element analysis of 3 internal fixations for distal type C3 femur fractures with medial wall bone defects.Zhong Nan Da Xue Xue Bao Yi Xue Ban. 2023 Nov 28;48(11):1711-1720. doi: 10.11817/j.issn.1672-7347.2023.230221. Zhong Nan Da Xue Xue Bao Yi Xue Ban. 2023. PMID: 38432862 Free PMC article. Chinese, English.
References
-
- Hill FW. A survey of bone fractures in the cat. J Small Anim Pract 1977; 18: 457-463. - PubMed
-
- Bookbinder PF, Flanders JA. Characteristics of pelvic fracture in the cat. Vet Comp Orthop Traumatol 1992; 37: 122-127.
-
- Voss K, Langley-Hobbs SJ, Montavon PM. Femur. In: Montavon PM, Voss K, Langley-Hobbs SJ. (eds). Feline orthopaedic surgery and musculoskeletal disease. Edinburgh: Saunders Elsevier, 2009, pp 455-474.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
